Matt Lentzner, Janine Jagger and I have designed a survey for participants of Gluten-free January, using the online application StatCrunch. Janine is an epidemiologist who studies healthcare worker safety at the University of Virginia; she has experience designing surveys for data collection so we're glad to have her on board. The survey will allow us to systematically gather and analyze data on the results of Gluten-free January. It will be 100 percent anonymous-- none of your answers will be connected to your identity in any way.
This survey has the potential to be really informative, but it will only work if you respond! The more people who take the survey, the more informative it will be, even if you didn't avoid gluten for a single day. If not very many people respond, it will be highly susceptible to "selection bias", where perhaps the only people who responded are people who improved the most, skewing the results.
Matt will be sending the survey out to everyone on his mailing list. Please complete it, even if you didn't end up avoiding gluten at all! There's no shame in it. The survey has responses built in for people who didn't avoid gluten. Your survey will still be useful!
We have potential data from over 500 people. After we crunch the numbers, I'll share them on the blog.
Monday, January 31, 2011
Eye Care Tips : Natural Remedies For Eye Care

Natural Eye Care Tips
# A diet rich in vitamin A sparkles the eyes. Vitamin A Foods are Papaya,fish, milk, eggs, cilantro and etc.
# Frequent washing of eyes with cold water also helps.
# For treating dark circles, cucumber slices on them is the best remedy.
# Massage with unscented castor oil is the best natural anti eye wrinkle remedy, even doctors suggest it.
# Overnight soaked amla and then washing the eyes next morning with this water is very helpful.
# Soaking cotton in slightly warm milk and covering your eyes with it for about 15 minutes is very beneficial.This will prevent the eye wrinkle forming under the eye.
# Massaging the scalp with curd soothes itchy and red eyes.
# For soothing tired eyes, dip two small cotton pads in very cold milk and place on closed eyes for approximately ten minutes and try to relax.
# For complete relaxation close your eyes and try thinking of pleasant and soothing things a little far away you may also concentrate on something at an arms length.
Consume food rich in Vitamin A, C and E as these act as antioxidants that helps the healthy flawless skin under the eye.
Sunday, January 30, 2011
Health In Old Age : How To Get Rid of Health Problems

Everyone wants to be healthy and vigorous throughout their life. But more so being healthy in old age is just like a boon. Since, old age brings with itself many health problems and if you are not taking complete care of yourself then these diseases becomes hard to cure and manage in old age. Here are given some useful health tips for old age:
Drink enough water:
It cleanses your body machinery and helps your heart in functioning well. Drinking of enough water will keep away chances of kidney stone and urine problem. It will also keep you looking young and active along with natural glow on your face.
Exercise regularly:
Inclusion of regular exercise in your daily life is the best health tips for old age. Exercising will not only help in promoting brain regeneration but also obviate decline in body parts. Practice any form on exercise depending on what you and your body can manage. Talk to you health care provider on what exercise you should undertake in your old age. Seniors can also use yoga which generates flexibility and balance in their body.
Well balanced diet:
Well balanced diet plays a very important part in keeping you healthy in old age. Avoid taking rich food like sweets, high stuffed and fried. As it will leave impact on your lever and may result in damaging it. You should add calcium rich diet as it will strengthen your bones. In old age teeth becomes week and so diet should also be soft cooked so that it intake is easy. Add fruits, vegetables and greens in your daily diet to maintain your health in old age. Proper nutritional food keeps many diseases away and also save you from common problems of aging. Addition of nutrition food can save from problem like obesity, cardiovascular diseases, diabetes and osteoporosis as these are generally prevalent nutrition related health problems which occur in old age.
Be happy and engage in recreational activities:
During old age, Factors like social isolation, low income and depression affect health in old age. Loneliness is a common problem in old age and leads to related problems. During this time, it becomes all the more important for seniors to take on some activity which occupy their time. Take part in social activities and indulge in pursuing your hobbies in spare time. Make friends and make use of their company to keep yourself active and happy.
Be happy and visit your doctor regularly:
During old age, seniors should take deep care of their health. This includes a regular visit to a health care professional. You should visit and consult your doctor regularly and try to implement all the suggestions and precautions given by your doctor.
Health in old age is not that hard to have and maintain. All you need is to follow some simple steps which can be easily included in your daily life without much effort. Most likely you are to know them already but now is the time to get started.
Beauty Tips For Women : Tips and How To Look Fabulous

These two Beauty Tips For Women that will help you to look fabulous and only take a short time to carry out.
Tip 1
To help keep your lips looking soft and moist apply some lip gloss to them as it contains ingredients that help to keep the lips hydrated. Also when away on holiday or even just out and about at home and the sun is shining don�t forget to apply products to the lips that also incorporate a sun cream in them.
Tip 2
To keep the look as natural as possible make sure that you use as little make up as possible. For the eyes opt for eye shadows in neutral colors and apply only mascara. As for your lips, use either a lip tint or gloss to help make them look more kissable. This is the kind of everyday look women should be going for when they only have a few minutes to get ready.
Thursday, January 27, 2011
The Diabetes Epidemic
The CDC just released its latest estimate of diabetes prevalence in the US (1):
These data are self-reported, and do not correct for differences in diagnosis methods, so they should be viewed with caution-- but they still serve to illustrate the trend. There was an increase in diabetes incidence that began in the early 1990s. More than 90 percent of cases are type 2 diabetics. Disturbingly, the trend does not show any signs of slowing.
The diabetes epidemic has followed on the heels of the obesity epidemic with 10-20 years of lag time. Excess body fat is the number one risk factor for diabetes*. As far as I can tell, type 2 diabetes is caused by insulin resistance, which is probably due to energy intake exceeding energy needs (overnutrition), causing a state of cellular insulin resistance as a defense mechanism to protect against the damaging effects of too much glucose and fatty acids (3). In addition, type 2 diabetes requires a predisposition that prevents the pancreatic beta cells from keeping up with the greatly increased insulin needs of an insulin resistant person**. Both factors are required, and not all insulin resistant people will develop diabetes as some people's beta cells are able to compensate by hypersecreting insulin.
Why does energy intake exceed energy needs in modern America and in most affluent countries? Why has the typical person's calorie intake increased by 250 calories per day since 1970 (4)? I believe it's because the fat mass "setpoint" has been increased, typically but not always by industrial food. I've been developing some new thoughts on this lately, and potentially new solutions, which I'll reveal when they're ready.
* In other words, it's the best predictor of future diabetes risk.
** Most of the common gene variants (of known function) linked with type 2 diabetes are thought to impact beta cell function (5).
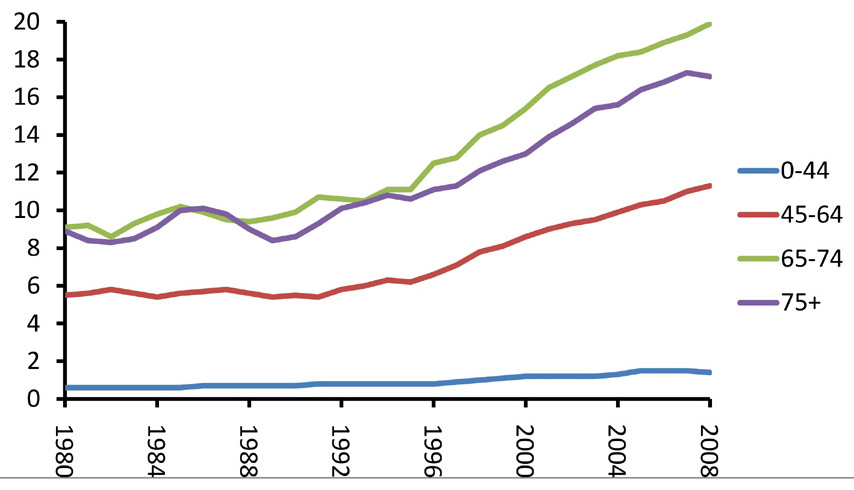
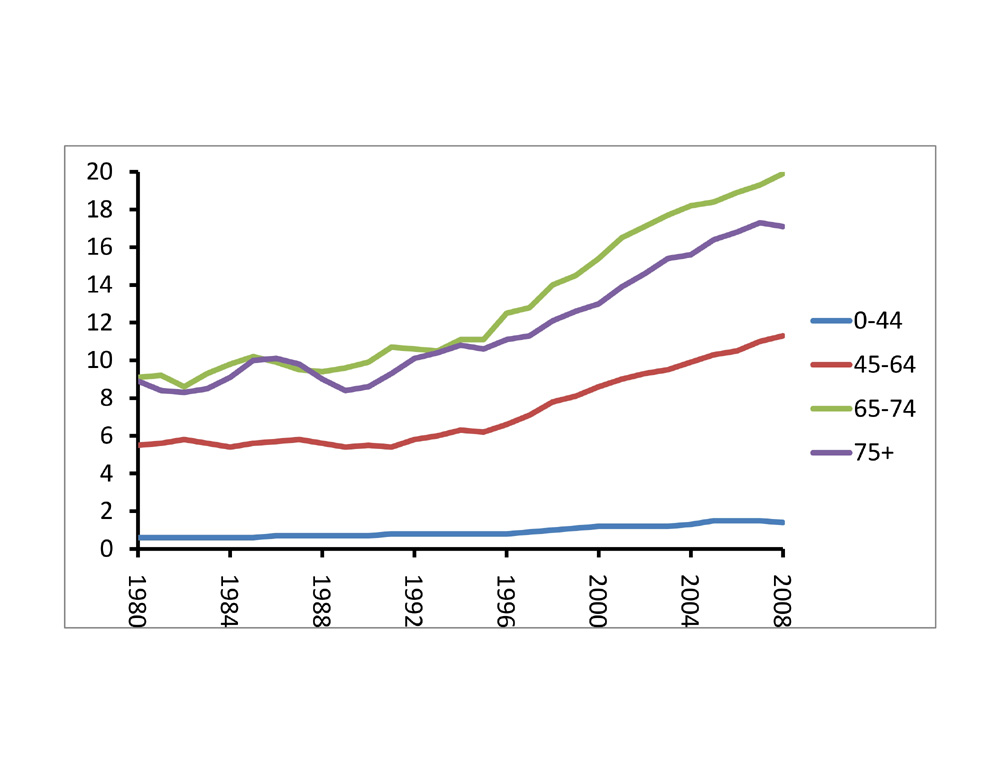
Diabetes affects 8.3 percent of Americans of all ages, and 11.3 percent of adults aged 20 and older, according to the National Diabetes Fact Sheet for 2011. About 27 percent of those with diabetes�7 million Americans�do not know they have the disease. Prediabetes affects 35 percent of adults aged 20 and older.Wow-- this is a massive problem. The prevalence of diabetes has been increasing over time, due to more people developing the disorder, improvements in diabetes care leading to longer survival time, and changes in the way diabetes is diagnosed. Here's a graph I put together based on CDC data, showing the trend of diabetes prevalence (percent) from 1980 to 2008 in different age categories (2):
These data are self-reported, and do not correct for differences in diagnosis methods, so they should be viewed with caution-- but they still serve to illustrate the trend. There was an increase in diabetes incidence that began in the early 1990s. More than 90 percent of cases are type 2 diabetics. Disturbingly, the trend does not show any signs of slowing.
{kind=link}
The diabetes epidemic has followed on the heels of the obesity epidemic with 10-20 years of lag time. Excess body fat is the number one risk factor for diabetes*. As far as I can tell, type 2 diabetes is caused by insulin resistance, which is probably due to energy intake exceeding energy needs (overnutrition), causing a state of cellular insulin resistance as a defense mechanism to protect against the damaging effects of too much glucose and fatty acids (3). In addition, type 2 diabetes requires a predisposition that prevents the pancreatic beta cells from keeping up with the greatly increased insulin needs of an insulin resistant person**. Both factors are required, and not all insulin resistant people will develop diabetes as some people's beta cells are able to compensate by hypersecreting insulin.
Why does energy intake exceed energy needs in modern America and in most affluent countries? Why has the typical person's calorie intake increased by 250 calories per day since 1970 (4)? I believe it's because the fat mass "setpoint" has been increased, typically but not always by industrial food. I've been developing some new thoughts on this lately, and potentially new solutions, which I'll reveal when they're ready.
* In other words, it's the best predictor of future diabetes risk.
** Most of the common gene variants (of known function) linked with type 2 diabetes are thought to impact beta cell function (5).
Two Wheat Challenge Ideas from Commenters
Some people have remarked that the blinded challenge method I posted is cumbersome.
Reader "Me" suggested:
Reader "Me" suggested:
You can buy wheat gluten in a grocery store. Why not simply have your friend add some wheat gluten to your normal protein shake.Reader David suggested:
They sell empty gelatin capsules with carob content to opacify them. Why not fill a few capsules with whole wheat flour, and then a whole bunch with rice starch or other placebo. For two weeks take a set of, say, three capsules every day, with the set of wheat capsules in line to be taken on a random day selected by your friend. This would further reduce the chances that you would see through the blind, and it prevent the risk of not being able to choke the "smoothie" down. It would also keep it to wheat and nothing but wheat (except for the placebo starch).The reason I chose the method in the last post is that it directly tests wheat in a form that a person would be likely to eat: bread. The limitation of the gluten shake method is that it would miss a sensitivity to components in wheat other than gluten. The limitation of the pill method is that raw flour is difficult to digest, so it would be difficult to extrapolate a sensitivity to cooked flour foods. You might be able to get around that by filling the pills with powdered bread crumbs. Those are two alternative ideas to consider if the one I posted seems too involved.
9 Things You Have To Know About Walking As Exercise
You know walking as exercise is good, but just could not squeeze it in your schedule?
Or you may have started a routine but got tired halfway?
You might be missing a lot!
There are lots of health benefits that one can get in walking for exercise. This is known to be a cure for ailments, makes stronger muscle and improves metabolism.
It is said that to get the best results; you must have a walking routine for a minimum of 40 minutes per day for 5 times a week.
There are many things you should understand about this type of exercise. Below are some examples...
9 Things You Have To Know About Walking As Exercise:
� Brisk Walking Burn Calories - you can burn excess calories by doing this exercise for at least 30 minutes a day, depending on the speed and weight of the person. For example, if a regular 125 lb person walks for 30 minutes with the speed of 3.5 mph a day, that person burns 108 calories. And if a 200 lb person does the same routine with the same speed and duration, he will lose 172 calories.
� Control Blood Pressure - University studies showed that walking is effective in decreasing the peak of blood pressure. A person who does their routine 3 days in a week helps their systolic blood pressure to decrease by 5 points.
� Memory Improvement - one benefit of this type of exercise in improving memory. Many research found out that as people grow older a part of the brain called "hippocampus" starts shrinking, which causes forgetfulness and memory loss. Walking helps in improving the memory by increasing the volume of hippocampus.
� Reduce Hip and Limb Fracture - it is a weight-bearing exercise that helps in increasing the density of the bones especially in the hips and lower back. As you grow older, this exercise will reduce the risk of hip and limb fracture.
� Decrease Depression - walking for exercise alerts chemical release in the brain linked to feeling happy, and calming it by raising the body temperature. This exercise will serve as a distraction, boost social interaction, and become a therapeutic form of relaxation.
� Control Type 2 Diabetes - it is said that physical activities are necessary in controlling type 2 diabetes. Walking routine plus a diet therapy is useful for patients with diabetes, since it decreases absolute hemoglobin value, improves insulin sensitivity and glycemic control.
� Good for Immune System - according to studies, this type of exercise helps in our body's immune system by fighting off viral illnesses like flu and colds. It is said that a moderate-paced routine between 30-40 minutes a day will increase the levels of immunity boosters present in the body.
� Increase Stamina - durability and air intake in the lungs are improved when you do this type of exercise routine. And it will make your heart stronger, power up your energy level, give your leg more strength and have an active lifestyle.
� Minimize Risk of Heart Attack - brisk walking can reduce the risk of heart diseases. Studies show that walking 1.5 miles a day cut the risk of having the disease in half compared to those who do not.
CV Vs Aerobics And Almonds Vs Cashews
Here are my bad numbers: My blood pressure is 109/70 and that is at the doctor's office. So I am nervous, waiting for my cancer blood tests results. I've seen it as low as 99 over 50s. My pulse runs as low as the 50s sometimes. How does one cite those as bad numbers? Those are athletic type numbers. That is the problem.
My LDL and total cholesterol are high. This is probably due in large part to heredity. AND MY LACK OF CV. Exercise that is. I have wondered why I can't get my cholesterol numbers where I want them. I have given up. So I asked my oncologist what I could do. My BP and pulse are so good. What could I possibly do better? I hike I bike I play tennis I do tai chi. I think nothing of climbing a thousand vertical feet.These are all great aerobically. My last oncologist would have nothing to do with discussing Lipid Panels. But this new friend told me to do 30 minutes of CV most days and eat almonds.
Isn't aerobics as good as CV? For some things yes. For some things aerobics is better.
But for flushing the arteries of LDL, moderate cardiovascular exercise is the only way to go. How did I not know? I never realized that I could be in good shape with a dangerous arterial flow issue.
Luckily my LDL is the large buoyant kind. Or the good bad kind. Yes now there is not just good and bad cholesterol but also GOOD AND BAD bad cholesterol. Got it? Here, it's easy. Divide your triglycerides by your HDL (or if you prefer divide HDL into triglycerides). If that number is 2 or less you are good. Less than 2 supposedly means large buoyant LDL (good) instead of small dense LDL (bad). My very bad numbers are 240 total and 170 LDL. My HDL is a little lower than I would like, as over 60 is optimal. My triglycerides are very low (probably thanks to aerobics). Anyway my triglyceride to HDL ratio is very good. I'm large and buoyant at 140 lbs.
Here's the thing: I think that my blood pressure and heartbeat are so low that I do not pump the cholesterol out of my arteries. "Why should we move even if we are buoyant?" they say. Well I don't like their attitude. I don't want an over abundance of any LDL and so now they will get moving with 30 minutes of cardiovascular moderate exercise most days, I hope. For me, at 60 years of age, that means a consistent pulse of 88 to 112. To get this formula subtract your age from 220. This leaves 160 for me. 55% to 70% of 160 is my moderate CV exercise number FOR A HALF HOUR STRAIGHT. I've worked much harder than this temporarily on a vertical climb or on a mountain bike, but not for 30 minutes straight. It should be "can't carry on a conversation, I'm gasping too hard through my mouth" for 30 minutes.
I will try to blow the LDL away. Hope it works.
Oh yeah, almonds. Did you know that what you eat doesn't have as much to do with cholesterol as you think? I do not even eat an average of 1/4 the "healthy" amount of cholesterol per day on my "anti-cancer" diet. Yet my cholesterol is high.My stupid liver is making the stupid stuff just like all of our stupid livers. Give the liver a brain will ya? It's so important that it could use one. So my liver is no doubt over producing. Oh yeah, almonds (a handful unsalted daily). They block LDL production. Not cashews buddy.
I want to proclaim "heredity schmeredity". I don't want to believe I can't beat genetics, at least partially.
I hate almonds. I love cashews. I hate moderate cardiovascular exercise. I love aerobics. Oh well, do what you are told. At least I can still have porter and garden fresh tomatoes (when my IBS isn't acting up).
Monday, January 24, 2011
Blinded Wheat Challenge
Self-experimentation can be an effective way to improve one's health*. One of the problems with diet self-experimentation is that it's difficult to know which changes are the direct result of eating a food, and which are the result of preconceived ideas about a food. For example, are you more likely to notice the fact that you're grumpy after drinking milk if you think milk makes people grumpy? Maybe you're grumpy every other day regardless of diet? Placebo effects and conscious/unconscious bias can lead us to erroneous conclusions.
The beauty of the scientific method is that it offers us effective tools to minimize this kind of bias. This is probably its main advantage over more subjective forms of inquiry**. One of the most effective tools in the scientific method's toolbox is a control. This is a measurement that's used to establish a baseline for comparison with the intervention, which is what you're interested in. Without a control measurement, the intervention measurement is typically meaningless. For example, if we give 100 people pills that cure belly button lint, we have to give a different group placebo (sugar) pills. Only the comparison between drug and placebo groups can tell us if the drug worked, because maybe the changing seasons, regular doctor's visits, or having your belly button examined once a week affects the likelihood of lint.
Another tool is called blinding. This is where the patient, and often the doctor and investigators, don't know which pills are placebo and which are drug. This minimizes bias on the part of the patient, and sometimes the doctor and investigators. If the patient knew he were receiving drug rather than placebo, that could influence the outcome. Likewise, investigators who aren't blinded while they're collecting data can unconsciously (or consciously) influence it.
Back to diet. I want to know if I react to wheat. I've been gluten-free for about a month. But if I eat a slice of bread, how can I be sure I'm not experiencing symptoms because I think I should? How about blinding and a non-gluten control?
Procedure for a Blinded Wheat Challenge
1. Find a friend who can help you.
2. Buy a loaf of wheat bread and a loaf of gluten-free bread.
3. Have your friend choose one of the loaves without telling you which he/she chose.
4. Have your friend take 1-3 slices, blend them with water in a blender until smooth. This is to eliminate differences in consistency that could allow you to determine what you're eating. Don't watch your friend do this-- you might recognize the loaf.
5. Pinch your nose and drink the "bread smoothie" (yum!). This is so that you can't identify the bread by taste. Rinse your mouth with water before releasing your nose. Record how you feel in the next few hours and days.
6. Wait a week. This is called a "washout period". Repeat the experiment with the second loaf, attempting to keep everything else about the experiment as similar as possible.
7. Compare how you felt each time. Have your friend "unblind" you by telling you which bread you ate on each day. If you experienced symptoms during the wheat challenge but not the control challenge, you may be sensitive to wheat.
If you want to take this to the next level of scientific rigor, repeat the procedure several times to see if the result is consistent. The larger the effect, the fewer times you need to repeat it to be confident in the result.
* Although it can also be disastrous. People who get into the most trouble are "extreme thinkers" who have a tendency to take an idea too far, e.g., avoid all animal foods, avoid all carbohydrate, avoid all fat, run two marathons a week, etc.
** More subjective forms of inquiry have their own advantages.
The beauty of the scientific method is that it offers us effective tools to minimize this kind of bias. This is probably its main advantage over more subjective forms of inquiry**. One of the most effective tools in the scientific method's toolbox is a control. This is a measurement that's used to establish a baseline for comparison with the intervention, which is what you're interested in. Without a control measurement, the intervention measurement is typically meaningless. For example, if we give 100 people pills that cure belly button lint, we have to give a different group placebo (sugar) pills. Only the comparison between drug and placebo groups can tell us if the drug worked, because maybe the changing seasons, regular doctor's visits, or having your belly button examined once a week affects the likelihood of lint.
Another tool is called blinding. This is where the patient, and often the doctor and investigators, don't know which pills are placebo and which are drug. This minimizes bias on the part of the patient, and sometimes the doctor and investigators. If the patient knew he were receiving drug rather than placebo, that could influence the outcome. Likewise, investigators who aren't blinded while they're collecting data can unconsciously (or consciously) influence it.
Back to diet. I want to know if I react to wheat. I've been gluten-free for about a month. But if I eat a slice of bread, how can I be sure I'm not experiencing symptoms because I think I should? How about blinding and a non-gluten control?
Procedure for a Blinded Wheat Challenge
1. Find a friend who can help you.
2. Buy a loaf of wheat bread and a loaf of gluten-free bread.
3. Have your friend choose one of the loaves without telling you which he/she chose.
4. Have your friend take 1-3 slices, blend them with water in a blender until smooth. This is to eliminate differences in consistency that could allow you to determine what you're eating. Don't watch your friend do this-- you might recognize the loaf.
5. Pinch your nose and drink the "bread smoothie" (yum!). This is so that you can't identify the bread by taste. Rinse your mouth with water before releasing your nose. Record how you feel in the next few hours and days.
6. Wait a week. This is called a "washout period". Repeat the experiment with the second loaf, attempting to keep everything else about the experiment as similar as possible.
7. Compare how you felt each time. Have your friend "unblind" you by telling you which bread you ate on each day. If you experienced symptoms during the wheat challenge but not the control challenge, you may be sensitive to wheat.
If you want to take this to the next level of scientific rigor, repeat the procedure several times to see if the result is consistent. The larger the effect, the fewer times you need to repeat it to be confident in the result.
* Although it can also be disastrous. People who get into the most trouble are "extreme thinkers" who have a tendency to take an idea too far, e.g., avoid all animal foods, avoid all carbohydrate, avoid all fat, run two marathons a week, etc.
** More subjective forms of inquiry have their own advantages.
Friday, January 21, 2011
Bed Bugs : How To Get Rid of Bed Bugs

Bedbugs have marched into shops, movie theaters, offices, and even opera houses, but their favorite breeding ground remains their namesake. As soon as you enter your hotel room (don't sprawl out on that plush bed just yet) inspect the sheets, mattress, and box spring, especially around the seams. You're looking for old skins (bedbugs shed papery layers that look like popcorn-kernel shells), black spots (bedbug poop), or the live insects themselves. If possible, stick your head under the bed and shine a flashlight on the bottom of the box spring.
Bedbugs love to hide in upholstered furniture. Wood chairs may be safer, but be wary of those with visible cracks. The critters can fit into any space that a credit card can be slipped into, says Jody Gangloff-Kaufmann, Ph.D., an entomologist at Cornell University. Pay particular attention to the seams as you carefully look between and beneath all cushions for bugs, empty skins, or feces.
When it comes to art, these parasites don't discriminate�they've been found around elegant oil paintings in expensive hotels and cheesy prints in seedy motels. If any art is hanging in your room, examine the frame closely and peer behind it for telltale signs.
Body heat is a bedbug magnet, and the pests have two hooklike claws on each of their six legs that allow them to hitch a ride on your clothes, says entomologist Jeffrey White. Never set your luggage on a hotel bed or floor; instead, give the suitcase rack a onceover before setting your bag on it as far from the bed as possible (it's best not to put it against a wall either). But don't unzip anything until you've checked out the rest of the room.
~source : womenshealthmag~
Thursday, January 20, 2011
Eating Wheat Gluten Causes Symptoms in Some People Who Don't Have Celiac Disease
Irritable bowel syndrome (IBS) is a condition characterized by the frequent occurrence of abdominal pain, diarrhea, constipation, bloating and/or gas. If that sounds like an extremely broad description, that's because it is. The word "syndrome" is medicalese for "we don't know what causes it." IBS seems to be a catch-all for various persistent digestive problems that aren't defined as separate disorders, and it has a very high prevalence: as high as 14 percent of people in the US, although the estimates depend on what diagnostic criteria are used (1). It can be brought on or exacerbated by several different types of stressors, including emotional stress and infection.
Mael�n Fontes Villalba at Lund University recently forwarded me an interesting new paper in the American Journal of Gastroenterology (2). Dr. Jessica R. Biesiekierski and colleagues recruited 34 IBS patients who did not have celiac disease, but who felt they had benefited from going gluten-free in their daily lives*. All patients continued on their pre-study gluten-free diet, however, all participants were provided with two slices of gluten-free bread and one gluten-free muffin per day. The investigators added isolated wheat gluten to the bread and muffins of half the study group.
During the six weeks of the intervention, patients receiving the gluten-free food fared considerably better on nearly every symptom of IBS measured. The most striking difference was in tiredness-- the gluten-free group was much less tired on average than the gluten group. Interestingly, they found that a negative reaction to gluten was not necessarily accompanied by the presence of anti-gluten antibodies in the blood, which is a test often used to diagnose gluten sensitivity.
Here's what I take away from this study:
I don't expect everyone to benefit from avoiding gluten. But for those who are really sensitive, it can make a huge difference. Digestive, autoimmune and neurological disorders associate most strongly with gluten sensitivity. Avoiding gluten can be a fruitful thing to try in cases of mysterious chronic illness. We're two-thirds of the way through Gluten-Free January. I've been fastidiously avoiding gluten, as annoying as it's been at times***. Has anyone noticed a change in their health?
* 56% of volunteers carried HLA-DQ2 or DQ8 alleles, which is slightly higher than the general population. Nearly all people with celiac disease carry one of these two alleles. 28% of volunteers were positive for anti-gliadin IgA, which is higher than the general population.
** Some people feel they are reacting to the fructans in wheat, rather than the gluten. If a modest amount of onion causes the same symptoms as eating wheat, then that may be true. If not, then it's probably the gluten.
*** I'm usually about 95% gluten-free anyway. But when I want a real beer, I want one brewed with barley. And when I want Thai food or sushi, I don't worry about a little bit of wheat in the soy sauce. If a friend makes me food with gluten in it, I'll eat it and enjoy it. This month I'm 100% gluten-free though, because I can't in good conscience encourage my blog readership to try it if I'm not doing it myself. At the end of the month, I'm going to do a blinded gluten challenge (with a gluten-free control challenge) to see once and for all if I react to it. Stay tuned for more on that.
Mael�n Fontes Villalba at Lund University recently forwarded me an interesting new paper in the American Journal of Gastroenterology (2). Dr. Jessica R. Biesiekierski and colleagues recruited 34 IBS patients who did not have celiac disease, but who felt they had benefited from going gluten-free in their daily lives*. All patients continued on their pre-study gluten-free diet, however, all participants were provided with two slices of gluten-free bread and one gluten-free muffin per day. The investigators added isolated wheat gluten to the bread and muffins of half the study group.
During the six weeks of the intervention, patients receiving the gluten-free food fared considerably better on nearly every symptom of IBS measured. The most striking difference was in tiredness-- the gluten-free group was much less tired on average than the gluten group. Interestingly, they found that a negative reaction to gluten was not necessarily accompanied by the presence of anti-gluten antibodies in the blood, which is a test often used to diagnose gluten sensitivity.
Here's what I take away from this study:
- Wheat gluten can cause symptoms in susceptible people who do not have celiac disease.
- A lack of circulating antibodies against gluten does not necessarily indicate a lack of gluten sensitivity.
- People with mysterious digestive problems may want to try avoiding gluten for a while to see if it improves their symptoms**.
- People with mysterious fatigue may want to try avoiding gluten.
I don't expect everyone to benefit from avoiding gluten. But for those who are really sensitive, it can make a huge difference. Digestive, autoimmune and neurological disorders associate most strongly with gluten sensitivity. Avoiding gluten can be a fruitful thing to try in cases of mysterious chronic illness. We're two-thirds of the way through Gluten-Free January. I've been fastidiously avoiding gluten, as annoying as it's been at times***. Has anyone noticed a change in their health?
* 56% of volunteers carried HLA-DQ2 or DQ8 alleles, which is slightly higher than the general population. Nearly all people with celiac disease carry one of these two alleles. 28% of volunteers were positive for anti-gliadin IgA, which is higher than the general population.
** Some people feel they are reacting to the fructans in wheat, rather than the gluten. If a modest amount of onion causes the same symptoms as eating wheat, then that may be true. If not, then it's probably the gluten.
*** I'm usually about 95% gluten-free anyway. But when I want a real beer, I want one brewed with barley. And when I want Thai food or sushi, I don't worry about a little bit of wheat in the soy sauce. If a friend makes me food with gluten in it, I'll eat it and enjoy it. This month I'm 100% gluten-free though, because I can't in good conscience encourage my blog readership to try it if I'm not doing it myself. At the end of the month, I'm going to do a blinded gluten challenge (with a gluten-free control challenge) to see once and for all if I react to it. Stay tuned for more on that.
Thursday, January 13, 2011
Does Dietary Saturated Fat Increase Blood Cholesterol? An Informal Review of Observational Studies
The diet-heart hypothesis states three things:
The relationship becomes much more complex when you consider lipoprotein subtypes, density and oxidation level, among other factors, but at the very least there is an association between habitual blood cholesterol level and heart attack risk. This is what you would want to see if your hypothesis states that high blood cholesterol causes heart attacks.
Now let's turn to the first contention, the hypothesis that dietary saturated fat increases serum cholesterol. This idea is so deeply ingrained in the scientific literature that many authors don't even bother providing references for it anymore. When references are provided, they nearly always point to the same type of study: short-term controlled diet trials, in which volunteers are fed different fats for 2-13 weeks and their blood cholesterol measured (2)*. These studies show that saturated fat increases both LDL cholesterol ("bad cholesterol") and HDL cholesterol ("good cholesterol"), but typically the former more than the latter. These are the studies on which the diet-heart hypothesis was built.
But now we have a problem. Nearly every high-quality (prospective) observational study ever conducted found that saturated fat intake is not associated with heart attack risk (3). So if saturated fat increases blood cholesterol, and higher blood cholesterol is associated with an increased risk of having a heart attack, then why don't people who eat more saturated fat have more heart attacks?
I'll begin to answer that question with another question: why do researchers almost never cite observational studies to support the idea that dietary saturated fat increases blood cholesterol? Surely if the hypothesis is correct, then people who habitually eat a lot of saturated fat should have high cholesterol, right? One reason may be that in most instances, when researchers have looked for a relationship between habitual saturated fat intake and blood cholesterol, it has been very small or nonexistent. Those findings are rarely cited, but let's have a look...
The Studies
It's difficult to do a complete accounting of these studies, but I've done my best to round them up. I can't claim this post is comprehensive, but I doubt I missed very many, and I certainly didn't exclude any that I came across. If you know of any I missed, please add them to the comments. [UPDATE 4-2012: I did miss several studies, although they're basically consistent with the conclusion I came to here. I plan to update this post with the new references at some point.]
The earliest and perhaps most interesting study I found was published in the British Medical Journal in 1963 and is titled "Diet and Plasma Cholesterol in 99 Bank Men" (4). Investigators asked volunteers to weigh all food consumed at home for 1-2 weeks, and describe in detail all food consumed away from home. Compliance was good. This dietary accounting method is much more accurate than in most observational studies today**. Animal fat intake ranged from 55 to 173 grams per day, and blood cholesterol ranged from 154 to 324 mg/dL, yet there was no relationship whatsoever between the two. I'm looking at a graph of animal fat intake vs. blood cholesterol as I write this, and it looks like someone shot it with a shotgun at 50 yards. They analyzed the data every which way, but were never able to squeeze even a hint of an association out of it:
The next study is the Bogalusa Heart Study, published in 1978, which studied the diet and health of 10 year old American children (8). This study found an association by one statistical method, and none by a second method****. They found that the dietary factors they analyzed explained no more than 4% of the variation in blood cholesterol. Overall, I think this study lends very little support to the hypothesis.
Next is the Western Electric study, published in 1981 (9). This study found an association between saturated fat intake and blood cholesterol in middle-aged men in Chicago. However, the correlation was small, and there was no association between saturated fat intake and heart attack deaths. They cited two other studies that found an association between dietary saturated fat and blood cholesterol (and did not cite any of the numerous studies that found no association). One was a very small study conducted in young men doing research in Antarctica, which did not measure saturated fat but found an association between total fat intake and blood cholesterol (10). The other studied Japanese (Nagasaki and Hiroshima) and Japanese Americans in Japan, Hawai'i and California respectively (11).
This study requires some discussion. Published in 1973, it found a correlation between saturated fat intake and blood cholesterol in Japan, Hawai'i but not in California. The strongest association was in Japan, where going from 5 to 75 g/day of saturated fat (a 15-fold change!) was associated with an increase in blood cholesterol from about 175 to 200 mg/dL. However, I don't think this study offers much support to the hypothesis upon closer examination. Food intake in Japan was collected by 24-hour recall in 1965-1967, when the diet was roughly 3/4 white rice by calories. The lower limit of saturated fat intake in Japan was 5g/day, 1/12th what was typically eaten in Hawai'i and California, and the Japanese average was 16g, with most people falling below 10g. That is an extraordinarily low saturated fat intake. I think a significant portion of the Japanese in this study, living in the war-ravaged cities of Nagasaki and Hiroshima, were over-reliant on white rice and had a very peculiar and perhaps deficient diet. Also, what is the difference between a diet with 5 and 75 grams of saturated fat per day? Those diets are probably very different, in many other ways than their saturated fat content.
In Japanese-Americans living in Hawai'i, over a range of saturated fat intakes between 5 and 110 g/day, cholesterol went from 210 to 220 mg/dL. That was statistically significant but it's not exactly knocking my socks off, considering it's a 22-fold difference in saturated fat intake. In California, going from 15 to 110 g/day of saturated fat (7.3-fold change) was not associated with a change in blood cholesterol. Blood cholesterol was 20-30 mg/dL lower in Japan than in Hawai'i or California at any given level of saturated fat intake (e.g., Japanese eating 30g per day vs. Hawai'ians eating 30g per day). I think it's probable that saturated fat is not the relevant factor here, or at least it's much less influential than other factors. An equally plausible explanation is that people in the very low range of saturated fat intake are the rural poor who eat a diet that differs in many ways from the diets at the upper end of the range, and other aspects of lifestyle such as physical activity also differ.
The most recent study was the Health Professional Follow-up study, published in 1996 (12). This was a massive, well funded study that found no relationship between saturated fat intake and blood cholesterol.
Conclusion
Of all the studies I came across, only the Western Electric study found a clear association between habitual saturated fat intake and blood cholesterol, and even that association was weak. The Bogalusa Heart study and the Japanese study provided inconsistent evidence for a weak association. The other studies I cited, including the bank workers' study, the Tecumseh study, the Evans county study, the Israel Ischemic Heart study, the Framingham study and the Health Professionals Follow-up study, found no association between the two factors.
Overall, the literature does not offer much support for the idea that long term saturated fat intake has a significant effect on the concentration of blood cholesterol in humans. If it's a factor at all, it must be rather weak. It may be that the diet-heart hypothesis rests in part on an over-reliance on the results of short-term controlled feeding studies. It would be nice to see this discussed more often (or at all) in the scientific literature. It is worth pointing out that the method used to collect diet information in most of these studies, the food frequency questionnaire, is not particularly accurate, so it's possible that there is a lot of variability inherent to the measurement that is partially masking an association. In any case, these controlled studies have typically shown that saturated fat increases both LDL and HDL, so even if saturated fat did have a modest long-term effect on blood cholesterol, as hinted at by some of the observational studies, its effect on heart attack risk would still be difficult to predict.
The Diet-heart Hypothesis: Stuck at the Starting Gate
Animal Models of Atherosclerosis: LDL
* As a side note, many of these studies were of poor quality, and were designed in ways that artificially inflated the effects of saturated fat on blood lipids. For example, using a run-in period high in linoleic acid, or comparing a saturated fat-rich diet to a linoleic acid-rich diet, and attributing the differences in blood cholesterol to the saturated fat. Some of them used hydrogenated seed oils as the saturated fat. Although not always consistent, I do think that overall these studies support the idea that saturated fat does have a modest ability to increase blood cholesterol in the short term.
** Although I would love to hear comments from anyone who has done controlled diet trials. I'm sure this method had flaws, as it was applied in the 1960s.
*** Reference cited in the Tecumseh paper: Kannel, W et al. The Framingham Study. An epidemiological Investigation of Cardiovascular Diseases. Section 24: The Framingham Diet Study: Diet and the Regulation of Serum Cholesterol. US Government Printing Office, 1970.
**** Table 5 shows that the Pearson correlation coefficient for saturated fat intake vs. blood cholesterol is not significant; table 6 shows that children in the two highest tertiles of blood cholesterol have a significantly higher intake of saturated fat, unsaturated fat, total fat and sodium than the lowest tertile. The relationship between saturated fat and blood cholesterol shows no evidence of dose-dependence (cholesterol tertiles= 15.6g, 18.4g, 18.5g saturated fat). The investigators did not attempt to adjust for confounding factors.
- Dietary saturated fat increases blood cholesterol
- Elevated blood cholesterol increases the risk of having a heart attack
- Therefore, dietary saturated fat increases the risk of having a heart attack
The relationship becomes much more complex when you consider lipoprotein subtypes, density and oxidation level, among other factors, but at the very least there is an association between habitual blood cholesterol level and heart attack risk. This is what you would want to see if your hypothesis states that high blood cholesterol causes heart attacks.
Now let's turn to the first contention, the hypothesis that dietary saturated fat increases serum cholesterol. This idea is so deeply ingrained in the scientific literature that many authors don't even bother providing references for it anymore. When references are provided, they nearly always point to the same type of study: short-term controlled diet trials, in which volunteers are fed different fats for 2-13 weeks and their blood cholesterol measured (2)*. These studies show that saturated fat increases both LDL cholesterol ("bad cholesterol") and HDL cholesterol ("good cholesterol"), but typically the former more than the latter. These are the studies on which the diet-heart hypothesis was built.
But now we have a problem. Nearly every high-quality (prospective) observational study ever conducted found that saturated fat intake is not associated with heart attack risk (3). So if saturated fat increases blood cholesterol, and higher blood cholesterol is associated with an increased risk of having a heart attack, then why don't people who eat more saturated fat have more heart attacks?
I'll begin to answer that question with another question: why do researchers almost never cite observational studies to support the idea that dietary saturated fat increases blood cholesterol? Surely if the hypothesis is correct, then people who habitually eat a lot of saturated fat should have high cholesterol, right? One reason may be that in most instances, when researchers have looked for a relationship between habitual saturated fat intake and blood cholesterol, it has been very small or nonexistent. Those findings are rarely cited, but let's have a look...
The Studies
It's difficult to do a complete accounting of these studies, but I've done my best to round them up. I can't claim this post is comprehensive, but I doubt I missed very many, and I certainly didn't exclude any that I came across. If you know of any I missed, please add them to the comments. [UPDATE 4-2012: I did miss several studies, although they're basically consistent with the conclusion I came to here. I plan to update this post with the new references at some point.]
The earliest and perhaps most interesting study I found was published in the British Medical Journal in 1963 and is titled "Diet and Plasma Cholesterol in 99 Bank Men" (4). Investigators asked volunteers to weigh all food consumed at home for 1-2 weeks, and describe in detail all food consumed away from home. Compliance was good. This dietary accounting method is much more accurate than in most observational studies today**. Animal fat intake ranged from 55 to 173 grams per day, and blood cholesterol ranged from 154 to 324 mg/dL, yet there was no relationship whatsoever between the two. I'm looking at a graph of animal fat intake vs. blood cholesterol as I write this, and it looks like someone shot it with a shotgun at 50 yards. They analyzed the data every which way, but were never able to squeeze even a hint of an association out of it:
Making the most out of the data in other ways- for example, by analysis of the men very stable in their diets, or in whom weighing of food intake was maximal, or where blood was taken close to the diet [measurement]- did not increase the correlation. Because the correlation coefficient is almost as often negative as positive, moreover, what is being discussed mostly is the absence of association, not merely association that is unexpectedly small.The next study to discuss is the 1976 Tecumseh study (5). This was a large cardiovascular observational study conducted in Tecumseh, Michigan, which is often used as the basis for comparison for other cardiovascular studies in the literature. Using the 24 hour dietary recall method, including an analysis of saturated fat, the investigators found that:
Cholesterol and triglyceride levels were unrelated to quality, quantity, or proportions of fat, carbohydrate or protein consumed in the 24-hr recall period.They also noted that the result was consistent with what had been reported in other previously published studies, including the Evans county study (6), the massive Israel Ischemic Heart Disease Study (7) and the Framingham study. One of the longest-running, most comprehensive and most highly cited observational studies, the Framingham study was organized by Harvard investigators and continues to this day. When investigators analyzed the relationship between saturated fat intake, serum cholesterol and heart attack risk, they were so disappointed that they never formally published the results. We know from multiple sources that they found no significant relationship between saturated fat intake and blood cholesterol or heart attack risk***.
The next study is the Bogalusa Heart Study, published in 1978, which studied the diet and health of 10 year old American children (8). This study found an association by one statistical method, and none by a second method****. They found that the dietary factors they analyzed explained no more than 4% of the variation in blood cholesterol. Overall, I think this study lends very little support to the hypothesis.
Next is the Western Electric study, published in 1981 (9). This study found an association between saturated fat intake and blood cholesterol in middle-aged men in Chicago. However, the correlation was small, and there was no association between saturated fat intake and heart attack deaths. They cited two other studies that found an association between dietary saturated fat and blood cholesterol (and did not cite any of the numerous studies that found no association). One was a very small study conducted in young men doing research in Antarctica, which did not measure saturated fat but found an association between total fat intake and blood cholesterol (10). The other studied Japanese (Nagasaki and Hiroshima) and Japanese Americans in Japan, Hawai'i and California respectively (11).
This study requires some discussion. Published in 1973, it found a correlation between saturated fat intake and blood cholesterol in Japan, Hawai'i but not in California. The strongest association was in Japan, where going from 5 to 75 g/day of saturated fat (a 15-fold change!) was associated with an increase in blood cholesterol from about 175 to 200 mg/dL. However, I don't think this study offers much support to the hypothesis upon closer examination. Food intake in Japan was collected by 24-hour recall in 1965-1967, when the diet was roughly 3/4 white rice by calories. The lower limit of saturated fat intake in Japan was 5g/day, 1/12th what was typically eaten in Hawai'i and California, and the Japanese average was 16g, with most people falling below 10g. That is an extraordinarily low saturated fat intake. I think a significant portion of the Japanese in this study, living in the war-ravaged cities of Nagasaki and Hiroshima, were over-reliant on white rice and had a very peculiar and perhaps deficient diet. Also, what is the difference between a diet with 5 and 75 grams of saturated fat per day? Those diets are probably very different, in many other ways than their saturated fat content.
In Japanese-Americans living in Hawai'i, over a range of saturated fat intakes between 5 and 110 g/day, cholesterol went from 210 to 220 mg/dL. That was statistically significant but it's not exactly knocking my socks off, considering it's a 22-fold difference in saturated fat intake. In California, going from 15 to 110 g/day of saturated fat (7.3-fold change) was not associated with a change in blood cholesterol. Blood cholesterol was 20-30 mg/dL lower in Japan than in Hawai'i or California at any given level of saturated fat intake (e.g., Japanese eating 30g per day vs. Hawai'ians eating 30g per day). I think it's probable that saturated fat is not the relevant factor here, or at least it's much less influential than other factors. An equally plausible explanation is that people in the very low range of saturated fat intake are the rural poor who eat a diet that differs in many ways from the diets at the upper end of the range, and other aspects of lifestyle such as physical activity also differ.
The most recent study was the Health Professional Follow-up study, published in 1996 (12). This was a massive, well funded study that found no relationship between saturated fat intake and blood cholesterol.
Conclusion
Of all the studies I came across, only the Western Electric study found a clear association between habitual saturated fat intake and blood cholesterol, and even that association was weak. The Bogalusa Heart study and the Japanese study provided inconsistent evidence for a weak association. The other studies I cited, including the bank workers' study, the Tecumseh study, the Evans county study, the Israel Ischemic Heart study, the Framingham study and the Health Professionals Follow-up study, found no association between the two factors.
Overall, the literature does not offer much support for the idea that long term saturated fat intake has a significant effect on the concentration of blood cholesterol in humans. If it's a factor at all, it must be rather weak. It may be that the diet-heart hypothesis rests in part on an over-reliance on the results of short-term controlled feeding studies. It would be nice to see this discussed more often (or at all) in the scientific literature. It is worth pointing out that the method used to collect diet information in most of these studies, the food frequency questionnaire, is not particularly accurate, so it's possible that there is a lot of variability inherent to the measurement that is partially masking an association. In any case, these controlled studies have typically shown that saturated fat increases both LDL and HDL, so even if saturated fat did have a modest long-term effect on blood cholesterol, as hinted at by some of the observational studies, its effect on heart attack risk would still be difficult to predict.
The Diet-heart Hypothesis: Stuck at the Starting Gate
Animal Models of Atherosclerosis: LDL
* As a side note, many of these studies were of poor quality, and were designed in ways that artificially inflated the effects of saturated fat on blood lipids. For example, using a run-in period high in linoleic acid, or comparing a saturated fat-rich diet to a linoleic acid-rich diet, and attributing the differences in blood cholesterol to the saturated fat. Some of them used hydrogenated seed oils as the saturated fat. Although not always consistent, I do think that overall these studies support the idea that saturated fat does have a modest ability to increase blood cholesterol in the short term.
** Although I would love to hear comments from anyone who has done controlled diet trials. I'm sure this method had flaws, as it was applied in the 1960s.
*** Reference cited in the Tecumseh paper: Kannel, W et al. The Framingham Study. An epidemiological Investigation of Cardiovascular Diseases. Section 24: The Framingham Diet Study: Diet and the Regulation of Serum Cholesterol. US Government Printing Office, 1970.
**** Table 5 shows that the Pearson correlation coefficient for saturated fat intake vs. blood cholesterol is not significant; table 6 shows that children in the two highest tertiles of blood cholesterol have a significantly higher intake of saturated fat, unsaturated fat, total fat and sodium than the lowest tertile. The relationship between saturated fat and blood cholesterol shows no evidence of dose-dependence (cholesterol tertiles= 15.6g, 18.4g, 18.5g saturated fat). The investigators did not attempt to adjust for confounding factors.
Tuesday, January 11, 2011
Dr. Fat
A blog reader recently made me a Wordle from Whole Health Source. A Wordle is a graphical representation of a text, where the size of each word represents how often it appears. Click on the image for a larger version.
 Apparently, the two most common words on this blog are "Dr" and "fat." It occurred to me that Dr. Fat would be a great nom de plume.
Apparently, the two most common words on this blog are "Dr" and "fat." It occurred to me that Dr. Fat would be a great nom de plume.
 Apparently, the two most common words on this blog are "Dr" and "fat." It occurred to me that Dr. Fat would be a great nom de plume.
Apparently, the two most common words on this blog are "Dr" and "fat." It occurred to me that Dr. Fat would be a great nom de plume.
Monday, January 3, 2011
Paleolithic Diet Clinical Trials, Part V
Dr. Staffan Lindeberg's group has published a new paleolithic diet paper in the journal Nutrition and Metabolism, titled "A Paleolithic Diet is More Satiating per Calorie than a Mediterranean-like Diet in Individuals with Ischemic Heart Disease" (1).
The data in this paper are from the same intervention as his group's 2007 paper in Diabetologia (2). To review the results of this paper, 12 weeks of a Paleolithic-style diet caused impressive fat loss and improvement in glucose tolerance, compared to 12 weeks of a Mediterranean-style diet, in volunteers with pre-diabetes or diabetes and ischemic heart disease. Participants who started off with diabetes ended up without it. A Paleolithic diet excludes grains, dairy, legumes and any other category of food that was not a major human food source prior to agriculture. I commented on this study a while back (3, 4).
One of the most intriguing findings in his 2007 study was the low calorie intake of the Paleolithic group. Despite receiving no instruction to reduce calorie intake, the Paleolithic group only ate 1,388 calories per day, compared to 1,823 calories per day for the Mediterranean group*. That's a remarkably low ad libitum calorie intake in the former (and a fairly low intake in the latter as well).
With such a low calorie intake over 12 weeks, you might think the Paleolithic group was starving. Fortunately, the authors had the foresight to measure satiety, or fullness, in both groups during the intervention. They found that satiety was almost identical in the two groups, despite the 24% lower calorie intake of the Paleolithic group. In other words, the Paleolithic group was just as full as the Mediterranean group, despite a considerably lower intake of calories. This implies to me that the body fat "set point" decreased, allowing a reduced calorie intake while body fat stores were burned to make up the calorie deficit. I suspect it also decreased somewhat in the Mediterranean group, although we can't know for sure because we don't have baseline satiety data for comparison.
There are a few possible explanations for this result. The first is that the Paleolithic group was eating more protein, a highly satiating macronutrient. However, given the fact that absolute protein intake was scarcely different between groups, I think this is unlikely to explain the reduced calorie intake.
A second possibility is that certain potentially damaging Neolithic foods (e.g., wheat and refined sugar) interfere with leptin signaling**, and removing them lowers fat mass by allowing leptin to function correctly. Dr. Lindeberg and colleagues authored a hypothesis paper on this topic in 2005 (5).
A third possibility is that a major dietary change of any kind lowers the body fat setpoint and reduces calorie intake for a certain period of time. In support of this hypothesis, both low-carbohydrate and low-fat diet trials show that overweight people spontaneously eat fewer calories when instructed to modify their diets in either direction (6, 7). More extreme changes may cause a larger decrease in calorie intake and fat mass, as evidenced by the results of low-fat vegan diet trials (8, 9). Chris Voigt's potato diet also falls into this category (10, 11). I think there may be something about changing food-related sensory cues that alters the defended level of fat mass. A similar idea is the basis of Seth Roberts' book The Shangri-La Diet.
If I had to guess, I would think the second and third possibilities contributed to the finding that Paleolithic dieters lost more fat without feeling hungry over the 12 week diet period.
*Intakes were determined using 4-day weighed food records.
**Leptin is a hormone produced by body fat that reduces food intake and increases energy expenditure by acting in the brain. The more fat a person carries, the more leptin they produce, and hypothetically this should keep body fat in a narrow window by this form of "negative feedback". Clearly, that's not the whole story, otherwise obesity wouldn't exist. A leading hypothesis is that resistance to the hormone leptin causes this feedback loop to defend a higher level of fat mass.
The data in this paper are from the same intervention as his group's 2007 paper in Diabetologia (2). To review the results of this paper, 12 weeks of a Paleolithic-style diet caused impressive fat loss and improvement in glucose tolerance, compared to 12 weeks of a Mediterranean-style diet, in volunteers with pre-diabetes or diabetes and ischemic heart disease. Participants who started off with diabetes ended up without it. A Paleolithic diet excludes grains, dairy, legumes and any other category of food that was not a major human food source prior to agriculture. I commented on this study a while back (3, 4).
One of the most intriguing findings in his 2007 study was the low calorie intake of the Paleolithic group. Despite receiving no instruction to reduce calorie intake, the Paleolithic group only ate 1,388 calories per day, compared to 1,823 calories per day for the Mediterranean group*. That's a remarkably low ad libitum calorie intake in the former (and a fairly low intake in the latter as well).
With such a low calorie intake over 12 weeks, you might think the Paleolithic group was starving. Fortunately, the authors had the foresight to measure satiety, or fullness, in both groups during the intervention. They found that satiety was almost identical in the two groups, despite the 24% lower calorie intake of the Paleolithic group. In other words, the Paleolithic group was just as full as the Mediterranean group, despite a considerably lower intake of calories. This implies to me that the body fat "set point" decreased, allowing a reduced calorie intake while body fat stores were burned to make up the calorie deficit. I suspect it also decreased somewhat in the Mediterranean group, although we can't know for sure because we don't have baseline satiety data for comparison.
There are a few possible explanations for this result. The first is that the Paleolithic group was eating more protein, a highly satiating macronutrient. However, given the fact that absolute protein intake was scarcely different between groups, I think this is unlikely to explain the reduced calorie intake.
A second possibility is that certain potentially damaging Neolithic foods (e.g., wheat and refined sugar) interfere with leptin signaling**, and removing them lowers fat mass by allowing leptin to function correctly. Dr. Lindeberg and colleagues authored a hypothesis paper on this topic in 2005 (5).
A third possibility is that a major dietary change of any kind lowers the body fat setpoint and reduces calorie intake for a certain period of time. In support of this hypothesis, both low-carbohydrate and low-fat diet trials show that overweight people spontaneously eat fewer calories when instructed to modify their diets in either direction (6, 7). More extreme changes may cause a larger decrease in calorie intake and fat mass, as evidenced by the results of low-fat vegan diet trials (8, 9). Chris Voigt's potato diet also falls into this category (10, 11). I think there may be something about changing food-related sensory cues that alters the defended level of fat mass. A similar idea is the basis of Seth Roberts' book The Shangri-La Diet.
If I had to guess, I would think the second and third possibilities contributed to the finding that Paleolithic dieters lost more fat without feeling hungry over the 12 week diet period.
*Intakes were determined using 4-day weighed food records.
**Leptin is a hormone produced by body fat that reduces food intake and increases energy expenditure by acting in the brain. The more fat a person carries, the more leptin they produce, and hypothetically this should keep body fat in a narrow window by this form of "negative feedback". Clearly, that's not the whole story, otherwise obesity wouldn't exist. A leading hypothesis is that resistance to the hormone leptin causes this feedback loop to defend a higher level of fat mass.
Subscribe to:
Posts (Atom)