I often focus on the bigger facets of the disease of civilization. Things like cardiovascular disease and cancer, which are major killers and the subject of intensive research. But the disease of civilization is a spectrum of disorders that affects the body in countless ways, large and small.
I recently read an interesting paper written by an all-star cast, including Loren Cordain, Staffan Lindeberg and Boyd Eaton. It's titled "Acne Vulgaris: A Disease of Western Civilization". The paper presents data from two different groups, the Kitavans of Papua New Guinea and the Ache hunter-gatherers of Paraguay. Both were systematically examined by doctors trained to diagnose acne. Out of 1,200 Kitavans and 115 Ache of all ages, not a single case of acne was observed. Hunter-gatherers and other healthy non-industrial cultures have nice skin. I dare you to find a pimple in Nutrition and Physical Degeneration.
In Western societies, acne is a fact of life. The paper states that 79 to 95% of modern adolescents suffer from some degree of acne, along with about 50% of young adults. That's an enormous difference.
The paper presents a very Cordain-esque hypothesis to explain the high incidence of acne in Western societies. In sum, they state that the Western diet causes hyperinsulinemia, which is thought to promote acne. This is due to insulin's effects on skin cell proliferation, its interference with the retinoid (vitamin A) signaling pathway, and its effect on sebum production.
They then proceed to point the finger at the glycemic index/load of the Western diet as the culprit behind hyperinsulinemia. It's an unsatisfying explanation because the Kitavans eat a diet that has a high glycemic load due to its high carbohydrate content, low fat content, and relatively high-glycemic index foods. I think the answer is more likely to reside in the specific types of carbohydrate (processed wheat) rather than their speed of digestion, with possible contributions from refined vegetable oil and an excessive sugar intake.
Monday, September 29, 2008
Thursday, September 25, 2008
Nonalcoholic Fatty Liver Disease
Nonalcoholic fatty liver disease (NAFLD) is milder form of NASH, in which the liver becomes enlarged and accumulates fat. Ready for a shocker? The prevalence of NAFLD is thought to be between 20 and 30 percent in the Western world, and rising. It's typically associated with insulin resistance and often with the metabolic syndrome. This has lead some researchers to believe it's caused by insulin resistance. It's a chicken and egg question, but I believe it's the other way around if anything.
There are certain animal models of human disease that are so informative I keep coming back to them again and again. One of my favorites is the LIRKO mouse, or liver-specific insulin receptor knockout mouse. The LIRKO mouse is missing its insulin receptor in the liver only, so it is a model of severe insulin resistance of the liver. It accumulates a small amount of fat in its liver in old age, but nothing that resembles NAFLD. So liver insulin resistance doesn't lead to NAFLD or NASH, at least in this model.
What else happens to the LIRKO mouse? It develops severe whole-body insulin resistance, impaired glucose tolerance, high fasting blood glucose and hyperinsulinemia (chronically elevated insulin). So insulin resistance in the liver is sufficient to cause whole-body insulin resistance, hyperinsulinemia and certain other hallmarks of the metabolic syndrome, while liver and whole-body insulin resistance are not sufficient to cause NAFLD or NASH. This is consistent with the fact that nearly everyone with NAFLD is insulin resistant, while many who are insulin resistant do not have NAFLD.
In all fairness, there are reasons why NAFLD is believed to be caused by insulin resistance. For example, insulin-sensitizing drugs improve NAFLD. However, that doesn't mean the initial metabolic 'hit' wasn't in the liver. One could imagine a scenario in which liver insulin resistance leads to insulin resistance in other tissues, which creates a positive feedback that aggravates NAFLD. Or perhaps NAFLD requires two 'hits', one to peripheral insulin sensitivity and another directly to the liver.
In any case, I feel that the most plausible mechanism for NAFLD goes something like this: too much n-6 from polyunsaturated vegetable oil (along with insufficient n-3), plus too much fructose from sweeteners, combine to cause NAFLD. The liver becomes insulin resistant at this point, leading to whole-body insulin resistance, hyperinsulinemia, impaired glucose tolerance and general metabolic havoc.
There are certain animal models of human disease that are so informative I keep coming back to them again and again. One of my favorites is the LIRKO mouse, or liver-specific insulin receptor knockout mouse. The LIRKO mouse is missing its insulin receptor in the liver only, so it is a model of severe insulin resistance of the liver. It accumulates a small amount of fat in its liver in old age, but nothing that resembles NAFLD. So liver insulin resistance doesn't lead to NAFLD or NASH, at least in this model.
What else happens to the LIRKO mouse? It develops severe whole-body insulin resistance, impaired glucose tolerance, high fasting blood glucose and hyperinsulinemia (chronically elevated insulin). So insulin resistance in the liver is sufficient to cause whole-body insulin resistance, hyperinsulinemia and certain other hallmarks of the metabolic syndrome, while liver and whole-body insulin resistance are not sufficient to cause NAFLD or NASH. This is consistent with the fact that nearly everyone with NAFLD is insulin resistant, while many who are insulin resistant do not have NAFLD.
In all fairness, there are reasons why NAFLD is believed to be caused by insulin resistance. For example, insulin-sensitizing drugs improve NAFLD. However, that doesn't mean the initial metabolic 'hit' wasn't in the liver. One could imagine a scenario in which liver insulin resistance leads to insulin resistance in other tissues, which creates a positive feedback that aggravates NAFLD. Or perhaps NAFLD requires two 'hits', one to peripheral insulin sensitivity and another directly to the liver.
In any case, I feel that the most plausible mechanism for NAFLD goes something like this: too much n-6 from polyunsaturated vegetable oil (along with insufficient n-3), plus too much fructose from sweeteners, combine to cause NAFLD. The liver becomes insulin resistant at this point, leading to whole-body insulin resistance, hyperinsulinemia, impaired glucose tolerance and general metabolic havoc.
Tuesday, September 23, 2008
Agave Syrup
Anna brought up agave syrup in a comment on the last post, so I thought I'd put up a little mini-post so everyone can benefit from what she pointed out.
Agave syrup is made from the heart of the agave plant, which is pressed to release a juice rich in inulin. Inulin is a polymer made of fructose molecules. The inulin is then broken down either by heat or by enzymatic processing. The result is a sweet syrup that is rich in fructose.
Agave syrup is marketed as a healthy, alternative sweetener. In fact, it's probably as bad or worse than high-fructose corn syrup (HFCS). They are both a refined and processed plant extract. Both are high in fructose, with agave syrup leading HFCS (estimates of agave syrup range up to 92% fructose by calories). Finally, agave syrup is expensive and inefficient to produce.
The high fructose content gives agave syrup a low glycemic index, because fructose does not raise blood glucose. Unfortunately, as some diabetics learned the hard way, using fructose as a substitute for sucrose (cane sugar) has negative long-term effects on insulin sensitivity.
In my opinion, sweeteners come with risks and there is no free lunch. The only solution is moderation.
Agave syrup is made from the heart of the agave plant, which is pressed to release a juice rich in inulin. Inulin is a polymer made of fructose molecules. The inulin is then broken down either by heat or by enzymatic processing. The result is a sweet syrup that is rich in fructose.
Agave syrup is marketed as a healthy, alternative sweetener. In fact, it's probably as bad or worse than high-fructose corn syrup (HFCS). They are both a refined and processed plant extract. Both are high in fructose, with agave syrup leading HFCS (estimates of agave syrup range up to 92% fructose by calories). Finally, agave syrup is expensive and inefficient to produce.
The high fructose content gives agave syrup a low glycemic index, because fructose does not raise blood glucose. Unfortunately, as some diabetics learned the hard way, using fructose as a substitute for sucrose (cane sugar) has negative long-term effects on insulin sensitivity.
In my opinion, sweeteners come with risks and there is no free lunch. The only solution is moderation.
Monday, September 22, 2008
How to Fatten Your Liver
Steatohepatitis is a condition in which the liver becomes inflamed and accumulates fat. It was formerly found almost exclusively in alcoholics. In the 1980s, a new condition was described called nonalcoholic steatohepatitis (NASH), basically steatohepatitis without the alcoholism. Today, NASH is thought to affect more than 2% of the adult American population. The liver has many important functions. It's not an organ you want to break.
This week, I've been reading about how to fatten your liver. First up: industrial vegetable oil. The study that initially sent me on this nerd safari was recently published in the Journal of Nutrition. It's titled "Increased Apoptosis in High-Fat Diet�Induced Nonalcoholic Steatohepatitis in Rats Is Associated with c-Jun NH2-Terminal Kinase Activation and Elevated Proapoptotic Bax". Quite a mouthful. The important thing for the purpose of this post is that the investigators fed rats a high-fat diet, which induced NASH.
Anytime a study mentions a "high-fat diet", I immediately look to see what they were actually feeding the animals. To my utter amazement, there was no information on the composition of the high-fat diet in the methods section, only a reference to another paper. Apparently fat composition is irrelevant. Despite the fact that a high-fat diet from coconut oil or butter does not produce NASH in rats. Fortunately, I was able to track down the reference. The only difference between the standard diet and the high-fat diet was the addition of a large amount of corn oil and the subtraction of carbohydrate (dextrin maltose).
Corn oil is one of the worst vegetable oils. You've eaten corn so you know it's not an oily seed. To concentrate the oil and make it palatable, manufacturers use organic solvents, high heat, and several rounds of chemical treatment. It's also extremely rich in n-6 linoleic acid. The consumption of corn oil and other n-6 rich oils has risen dramatically in the US in the last 30 years, making them prime suspects in NASH. They have replaced the natural (more saturated) fats we once got from meat and milk.
Next up: fructose. Feeding rats an extreme amount of fructose (60% of calories) gives them nonalcoholic fatty liver disease (NAFLD), NASH's younger sibling, even when the fat in their chow is lard. Given the upward trend of US fructose consumption (mostly from high-fructose corn syrup), and the refined sugar consumed everywhere else (50% fructose), it's also high on my list of suspects.
Here's my prescription for homemade foie gras: take one serving of soybean oil fried french fries, a basket of corn oil fried chicken nuggets, a healthy salad drenched in cottonseed oil ranch dressing, and wash it all down with a tall cup of soda. It's worked for millions of Americans!
This week, I've been reading about how to fatten your liver. First up: industrial vegetable oil. The study that initially sent me on this nerd safari was recently published in the Journal of Nutrition. It's titled "Increased Apoptosis in High-Fat Diet�Induced Nonalcoholic Steatohepatitis in Rats Is Associated with c-Jun NH2-Terminal Kinase Activation and Elevated Proapoptotic Bax". Quite a mouthful. The important thing for the purpose of this post is that the investigators fed rats a high-fat diet, which induced NASH.
Anytime a study mentions a "high-fat diet", I immediately look to see what they were actually feeding the animals. To my utter amazement, there was no information on the composition of the high-fat diet in the methods section, only a reference to another paper. Apparently fat composition is irrelevant. Despite the fact that a high-fat diet from coconut oil or butter does not produce NASH in rats. Fortunately, I was able to track down the reference. The only difference between the standard diet and the high-fat diet was the addition of a large amount of corn oil and the subtraction of carbohydrate (dextrin maltose).
Corn oil is one of the worst vegetable oils. You've eaten corn so you know it's not an oily seed. To concentrate the oil and make it palatable, manufacturers use organic solvents, high heat, and several rounds of chemical treatment. It's also extremely rich in n-6 linoleic acid. The consumption of corn oil and other n-6 rich oils has risen dramatically in the US in the last 30 years, making them prime suspects in NASH. They have replaced the natural (more saturated) fats we once got from meat and milk.
Next up: fructose. Feeding rats an extreme amount of fructose (60% of calories) gives them nonalcoholic fatty liver disease (NAFLD), NASH's younger sibling, even when the fat in their chow is lard. Given the upward trend of US fructose consumption (mostly from high-fructose corn syrup), and the refined sugar consumed everywhere else (50% fructose), it's also high on my list of suspects.
Here's my prescription for homemade foie gras: take one serving of soybean oil fried french fries, a basket of corn oil fried chicken nuggets, a healthy salad drenched in cottonseed oil ranch dressing, and wash it all down with a tall cup of soda. It's worked for millions of Americans!
Thursday, September 18, 2008
A New Toy
I bought a new toy the other day: a blood glucose meter. I was curious about my post-meal blood glucose after my HbA1c reading came back higher than I was expecting. A blood glucose meter is the only way to know what your blood sugar is doing in your normal setting.
"Glucose intolerance" is the inability to effectively control blood glucose as it enters the bloodstream from the digestive system. It results in elevated blood sugar after eating carbohydrate, which is not a good thing. In someone with normal glucose tolerance, insulin is secreted in sufficient amounts, and the tissues are sufficiently sensitive to it, that blood glucose is kept within a fairly tight range of concentrations.
Glucose tolerance is typically the first thing to deteriorate in the process leading to type II diabetes. By the time fasting glucose is elevated, glucose intolerance is usually well established. Jenny Ruhl talks about this in her wonderful book Blood Sugar 101. Unfortunately, fasting glucose is the most commonly administered glucose test. That's because the more telling one, the oral glucose tolerance test (OGTT), is more involved and more expensive.
An OGTT involves drinking a concentrated solution of glucose and monitoring blood glucose at one and two hours. Values of >140 mg/dL at one hour and >120 mg/dL at two hours are considered "normal". If you have access to a blood glucose meter, you can give yourself a makeshift OGTT. You eat 60-70 grams of quickly-digesting carbohydrate with no fat to slow down absorption and monitor your glucose.
I gave myself an OGTT tonight. I ate a medium-sized boiled potato and a large slice of white bread, totaling about 60g of carbohydrate. Potatoes and bread digest very quickly, resulting in a blood glucose spike similar to drinking concentrated glucose! You can see that in the graph below. I ate at time zero. By 15 minutes, my blood glucose had reached its peak at 106 mg/dL.

My numbers were 97 mg/dL at one hour, and 80 mg/dL at two hours; far below the cutoff for impaired glucose tolerance. I completely cleared the glucose by an hour and 45 minutes. My maximum value was 106 mg/dL, also quite good. That's despite the fact that I used more carbohydrate for the OGTT than I would typically eat in a sitting. I hope you like the graph; I had to prick my fingers 10 times to make it! I thought it would look good with a lot of data points.
I'm going to have fun with this glucose meter. I've already gotten some valuable information. For example, just as I suspected, fast-digesting carbohydrate is not a problem for someone with a well-functioning pancreas and insulin-sensitive tissues. This is consistent with what we see in the Kitavans, who eat a high-carbohydrate, high glycemic load diet, yet are extremely healthy. Of course, for someone with impaired glucose tolerance (very common in industrial societies), fast-digesting carbohydrates could be the kiss of death. The big question is, what causes the pancreas to deteriorate and the tissues to become insulin resistant? Considering certain non-industrial societies were eating plenty of carbohydrate with no problems, it must be something about the modern lifestyle: industrially processed grains (particularly wheat), industrial vegetable oils, refined sugar, lack of fat-soluble vitamins, toxic pollutants and inactivity come to mind. One could make a case for any of those factors contributing to the problem.
"Glucose intolerance" is the inability to effectively control blood glucose as it enters the bloodstream from the digestive system. It results in elevated blood sugar after eating carbohydrate, which is not a good thing. In someone with normal glucose tolerance, insulin is secreted in sufficient amounts, and the tissues are sufficiently sensitive to it, that blood glucose is kept within a fairly tight range of concentrations.
Glucose tolerance is typically the first thing to deteriorate in the process leading to type II diabetes. By the time fasting glucose is elevated, glucose intolerance is usually well established. Jenny Ruhl talks about this in her wonderful book Blood Sugar 101. Unfortunately, fasting glucose is the most commonly administered glucose test. That's because the more telling one, the oral glucose tolerance test (OGTT), is more involved and more expensive.
An OGTT involves drinking a concentrated solution of glucose and monitoring blood glucose at one and two hours. Values of >140 mg/dL at one hour and >120 mg/dL at two hours are considered "normal". If you have access to a blood glucose meter, you can give yourself a makeshift OGTT. You eat 60-70 grams of quickly-digesting carbohydrate with no fat to slow down absorption and monitor your glucose.
I gave myself an OGTT tonight. I ate a medium-sized boiled potato and a large slice of white bread, totaling about 60g of carbohydrate. Potatoes and bread digest very quickly, resulting in a blood glucose spike similar to drinking concentrated glucose! You can see that in the graph below. I ate at time zero. By 15 minutes, my blood glucose had reached its peak at 106 mg/dL.

My numbers were 97 mg/dL at one hour, and 80 mg/dL at two hours; far below the cutoff for impaired glucose tolerance. I completely cleared the glucose by an hour and 45 minutes. My maximum value was 106 mg/dL, also quite good. That's despite the fact that I used more carbohydrate for the OGTT than I would typically eat in a sitting. I hope you like the graph; I had to prick my fingers 10 times to make it! I thought it would look good with a lot of data points.
I'm going to have fun with this glucose meter. I've already gotten some valuable information. For example, just as I suspected, fast-digesting carbohydrate is not a problem for someone with a well-functioning pancreas and insulin-sensitive tissues. This is consistent with what we see in the Kitavans, who eat a high-carbohydrate, high glycemic load diet, yet are extremely healthy. Of course, for someone with impaired glucose tolerance (very common in industrial societies), fast-digesting carbohydrates could be the kiss of death. The big question is, what causes the pancreas to deteriorate and the tissues to become insulin resistant? Considering certain non-industrial societies were eating plenty of carbohydrate with no problems, it must be something about the modern lifestyle: industrially processed grains (particularly wheat), industrial vegetable oils, refined sugar, lack of fat-soluble vitamins, toxic pollutants and inactivity come to mind. One could make a case for any of those factors contributing to the problem.
Friday, September 12, 2008
Inactivity and Weight Gain
Most of the papers I read in the field pay lip-service to some familiar stories: thrifty genes; calories in, calories out; energy density; fat intake; gluttony and sloth.
It may sound counterintuitive, but how do we know that inactivity causes overweight and not the other way around? In other words, isn't it possible that metabolic deregulation could cause both overweight and a reduced activity level? The answer is clearly yes. There are a number of hormones and other factors that influence activity level in animals and humans. For example, the "Zucker fatty" rat, a genetic model of severe leptin resistance, is obese and hypoactive (I wrote about it here). It's actually a remarkable facsimile of the metabolic syndrome. Since leptin resistance typically comes before insulin resistance and predicts the metabolic syndrome, modern humans may be going through a process similar to the Zucker rat.
Back to the paper. Dr. Nicholas Wareham and his group followed 393 healthy white men for 5.6 years. They took baseline measurements of body composition (weight, BMI and waist circumference) and activity level, and then measured the same things after 5.6 years. In a nutshell, here's what they found:
It may sound counterintuitive, but how do we know that inactivity causes overweight and not the other way around? In other words, isn't it possible that metabolic deregulation could cause both overweight and a reduced activity level? The answer is clearly yes. There are a number of hormones and other factors that influence activity level in animals and humans. For example, the "Zucker fatty" rat, a genetic model of severe leptin resistance, is obese and hypoactive (I wrote about it here). It's actually a remarkable facsimile of the metabolic syndrome. Since leptin resistance typically comes before insulin resistance and predicts the metabolic syndrome, modern humans may be going through a process similar to the Zucker rat.
Back to the paper. Dr. Nicholas Wareham and his group followed 393 healthy white men for 5.6 years. They took baseline measurements of body composition (weight, BMI and waist circumference) and activity level, and then measured the same things after 5.6 years. In a nutshell, here's what they found:
- Sedentary time associates with overweight at any given timepoint. This is consistent with other studies.
- Overweight at the beginning of the study predicted inactivity after 5.6 years.
- Inactivity at the beginning of the study was not associated with overweight at the end.
Monday, September 8, 2008
A Practical Approach to Omega Fats
Hunter-gatherers and healthy non-industrial cultures didn't know what omega-6 and omega-3 fats were. They didn't balance nutrients precisely; they stayed healthy by eating foods that they knew were available and nourishing. Therefore, I don't think it's necessary to bean count omega fats, and I don't think there's likely to be a single ideal ratio of n-6 to n-3. However, I do think there's evidence for an optimal range. To find out what it is, let's look at what's been done by healthy cultures in the past:
I think there's a simple way to interpret all this. Number one, don't eat vegetable oils high in n-6 fats. They are mostly industrial creations that have never supported human health. Number two, find a source of n-3 fats that can approximately balance your n-6 intake. In practical terms, this means minimizing sources of n-6 and eating modest amounts of n-3 to balance it. Some foods are naturally balanced, such as grass-fed dairy and pastured lamb. Others, like coconut oil, have so little n-6 it doesn't take much n-3 to create a proper balance.
Animal sources of n-3 are the best because they provide pre-formed long-chain fats like DHA, which some people have difficulty producing themselves. Flax oil may have some benefits as well. Fish oil and cod liver oil can be a convenient source of n-3; take them in doses of one teaspoon or less. As usual, whole foods are probably better than isolated oils. Weston Price noted that cultures throughout the world went to great lengths to obtain fresh and dried marine foods. Choose shellfish and wild fish that are low on the food chain so they aren't excessively polluted.
I don't think adding gobs of fish oil on top of the standard American diet to correct a poor n-6:n-3 ratio is optimal. It may be better than no fish oil, but it's probably not the best approach. I just read a study, hot off the presses, that examines this very issue in young pigs. Pigs are similar to humans in many ways, including aspects of their fat metabolism. They were fed three diets: a "deficient" diet containing some n-6 but very little n-3; a "contemporary" diet containing a lot of n-6 and some n-3; an "evolutionary" diet containing a modest, balanced amount of n-6 and n-3; and a "supplemented" diet, which is the contemporary diet plus DHA and arachidonic acid (AA).
Using the evolutionary diet as a benchmark, none of the other diets were able to achieve the same fatty acid profile in the young pigs' brains, blood, liver or heart. They also showed that neurons in culture require DHA for proper development, and excess n-6 interferes with the process.
With that said, here are a few graphs of the proportion of n-6 in common foods. These numbers all come from nutrition data. They reflect the percentage n-6 out of the total fat content. First, animal fats:
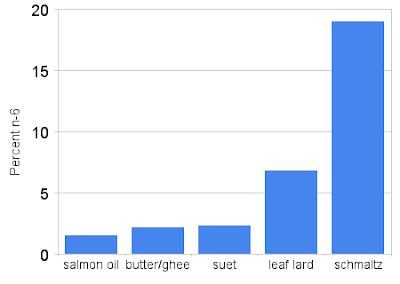 Except salmon oil, these are traditional fats suitable for cooking. Except schmaltz (chicken fat), they are relatively low in n-6. Next, vegetable oils:
Except salmon oil, these are traditional fats suitable for cooking. Except schmaltz (chicken fat), they are relatively low in n-6. Next, vegetable oils:
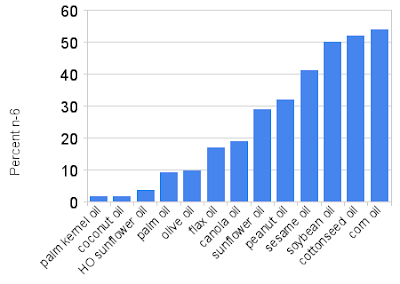 These range from very low in n-6 to very high. Most of the modern, industrially processed oils are on the right, while most traditional oils are on the left. I don't recommend using anything to the right of olive oil on a regular basis. "HO" sunflower oil is high-oleic, which means it has been bred for a high monounsaturated fat content at the expense of n-6. Here are the meats and eggs:
These range from very low in n-6 to very high. Most of the modern, industrially processed oils are on the right, while most traditional oils are on the left. I don't recommend using anything to the right of olive oil on a regular basis. "HO" sunflower oil is high-oleic, which means it has been bred for a high monounsaturated fat content at the expense of n-6. Here are the meats and eggs:
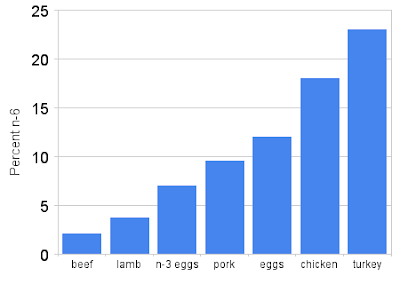 n-3 eggs are from hens fed flax or seaweed, while the other bar refers to conventional eggs.
n-3 eggs are from hens fed flax or seaweed, while the other bar refers to conventional eggs.
A few of these foods are good sources of n-3. At the top of the list is fish oil, followed by n-3 eggs, grass-fed butter, and the fat of grass-fed ruminants. It is possible to keep a good balance without seafood, it just requires keeping n-6 fats to an absolute minimum. It's also possible to overdo n-3 fats. The traditional Inuit, despite their good overall health, did not clot well. They commonly developed nosebleeds that would last for three days, for example. This is thought to be due to the effect of n-3 on blood clotting. But keep in mind that their n-3 intake was so high it would be difficult to achieve today without drinking wine glasses full of fish oil.
- Hunter-gatherers living mostly on land animals: 2:1 to 4:1
- Pacific islanders getting most of their fat from coconut and fish: 1:2
- Inuit and other Pacific coast Americans: 1:4 or less
- Dairy-based cultures: 1:1 to 2:1
- Cultures eating fish and grains: 1:2 or less
I think there's a simple way to interpret all this. Number one, don't eat vegetable oils high in n-6 fats. They are mostly industrial creations that have never supported human health. Number two, find a source of n-3 fats that can approximately balance your n-6 intake. In practical terms, this means minimizing sources of n-6 and eating modest amounts of n-3 to balance it. Some foods are naturally balanced, such as grass-fed dairy and pastured lamb. Others, like coconut oil, have so little n-6 it doesn't take much n-3 to create a proper balance.
Animal sources of n-3 are the best because they provide pre-formed long-chain fats like DHA, which some people have difficulty producing themselves. Flax oil may have some benefits as well. Fish oil and cod liver oil can be a convenient source of n-3; take them in doses of one teaspoon or less. As usual, whole foods are probably better than isolated oils. Weston Price noted that cultures throughout the world went to great lengths to obtain fresh and dried marine foods. Choose shellfish and wild fish that are low on the food chain so they aren't excessively polluted.
I don't think adding gobs of fish oil on top of the standard American diet to correct a poor n-6:n-3 ratio is optimal. It may be better than no fish oil, but it's probably not the best approach. I just read a study, hot off the presses, that examines this very issue in young pigs. Pigs are similar to humans in many ways, including aspects of their fat metabolism. They were fed three diets: a "deficient" diet containing some n-6 but very little n-3; a "contemporary" diet containing a lot of n-6 and some n-3; an "evolutionary" diet containing a modest, balanced amount of n-6 and n-3; and a "supplemented" diet, which is the contemporary diet plus DHA and arachidonic acid (AA).
Using the evolutionary diet as a benchmark, none of the other diets were able to achieve the same fatty acid profile in the young pigs' brains, blood, liver or heart. They also showed that neurons in culture require DHA for proper development, and excess n-6 interferes with the process.
With that said, here are a few graphs of the proportion of n-6 in common foods. These numbers all come from nutrition data. They reflect the percentage n-6 out of the total fat content. First, animal fats:
 Except salmon oil, these are traditional fats suitable for cooking. Except schmaltz (chicken fat), they are relatively low in n-6. Next, vegetable oils:
Except salmon oil, these are traditional fats suitable for cooking. Except schmaltz (chicken fat), they are relatively low in n-6. Next, vegetable oils: These range from very low in n-6 to very high. Most of the modern, industrially processed oils are on the right, while most traditional oils are on the left. I don't recommend using anything to the right of olive oil on a regular basis. "HO" sunflower oil is high-oleic, which means it has been bred for a high monounsaturated fat content at the expense of n-6. Here are the meats and eggs:
These range from very low in n-6 to very high. Most of the modern, industrially processed oils are on the right, while most traditional oils are on the left. I don't recommend using anything to the right of olive oil on a regular basis. "HO" sunflower oil is high-oleic, which means it has been bred for a high monounsaturated fat content at the expense of n-6. Here are the meats and eggs: n-3 eggs are from hens fed flax or seaweed, while the other bar refers to conventional eggs.
n-3 eggs are from hens fed flax or seaweed, while the other bar refers to conventional eggs. A few of these foods are good sources of n-3. At the top of the list is fish oil, followed by n-3 eggs, grass-fed butter, and the fat of grass-fed ruminants. It is possible to keep a good balance without seafood, it just requires keeping n-6 fats to an absolute minimum. It's also possible to overdo n-3 fats. The traditional Inuit, despite their good overall health, did not clot well. They commonly developed nosebleeds that would last for three days, for example. This is thought to be due to the effect of n-3 on blood clotting. But keep in mind that their n-3 intake was so high it would be difficult to achieve today without drinking wine glasses full of fish oil.
Saturday, September 6, 2008
Omega Fats and Cardiovascular Disease
I noticed something strange when I was poring over data about the Inuit last month. Modern Inuit who have adopted Western food habits get fat, they get diabetes... but they don't get heart attacks. This was a paradox to me at the time, because heart disease mortality typically comes along with the cluster of modern, non-communicable diseases I call the "diseases of civilization".
One of the interesting things about the modern Inuit diet is it's most often a combination of Western and traditional foods. For example, they typically use white flour and sugar, but continue to eat seal oil and fish. Both seal oil and fish are a concentrated source of long-chain omega-3 (n-3) fatty acids.The 'paradox' makes much more sense to me now that I've seen this:
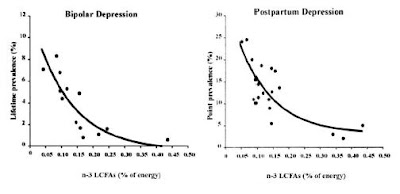
 It's from the same paper as the graphs in the last post. Note that it doesn't take much n-3 to get you to the asymptote. Here's another one that might interest you:
It's from the same paper as the graphs in the last post. Note that it doesn't take much n-3 to get you to the asymptote. Here's another one that might interest you:
 The finding in this graph is supported by the Lyon diet heart study, which I'll describe below. One more graph from a presentation by Dr. Lands, since I began by talking about the Inuit:
The finding in this graph is supported by the Lyon diet heart study, which I'll describe below. One more graph from a presentation by Dr. Lands, since I began by talking about the Inuit:

Cardiovascular disease mortality tracks well with the n-6 content of blood plasma, both across populations and within them. You can see modern Quebec Inuit have the same low rate of CVD mortality as the Japanese. The five red triangles are from MRFIT, a large American intervention trial. They represent the study participants divided into five groups based on their plasma n-6. Note that the average percentage of n-6 fatty acids is very high, even though the trial occurred in the 1970s! Since n-3 and n-6 fats compete for space in human tissue, it makes sense that the Inuit are protected from CVD by their high n-3 intake. [Update: I don't read too much into this graph because there are so may confounding variables. It's an interesting observation, but take it with a grain of salt.. SJG 2011].
Now for a little mechanism. Dr. Lands' hypothesis is that a high n-6 intake promotes a general state of inflammation in the body. The term 'inflammation' refers to the chronic activation of the innate immune system. The reason is that n-3 and n-6 fats are precursors to longer-chain signaling molecules called eicosanoids. In a nutshell, eicosanoids produced from n-6 fatty acids are more inflammatory and promote thrombosis (clotting) more than those produced from n-3 fatty acids. Dr. Lands is in a position to know this, since he was one of the main researchers involved in discovering these mechanisms. He points out that taking aspirin to 'thin' the blood and reduce inflammation (by inhibiting inflammatory eicosanoids) basically puts a band-aid over the problem caused by excess n-6 fats to begin with. [Update- this mechanism turns out not to be so straightforward. SJG 2011]
The Lyon Diet Heart Study assessed the effect of n-3 fat supplementation on CVD risk. The four-year intervention involved a number of diet changes designed to mimic the American Heart Association's concept of a "Mediterranean diet". The participants were counseled to eat a special margarine that was high in n-3 from alpha-linolenic acid. Overall PUFA intake decreased, mostly due to n-6 reduction, and n-3 intake increased relative to controls. The intervention caused a 70% reduction in cardiac mortality and a large reduction in all-cause mortality, a smashing success by any measure.
In a large five-year intervention trial in Japan, JELIS, patients who took EPA (a long-chain n-3 fatty acid) plus statins had 19% fewer cardiac events than patients taking statins alone. I don't know why you would give EPA by itself when it occurs with DHA and alpha-linolenic acid in nature, but it did nevertheless have a significant effect. Keep in mind that this trial was in Japan, where they already have a much better n-6/n-3 ratio than in Western nations.
In my opinion, what all the data (including a lot that I haven't included) point to is that a good n-6 to n-3 ratio may be important for vibrant health and proper development. In the next post, I'll talk about practical considerations for achieving a good ratio.
One of the interesting things about the modern Inuit diet is it's most often a combination of Western and traditional foods. For example, they typically use white flour and sugar, but continue to eat seal oil and fish. Both seal oil and fish are a concentrated source of long-chain omega-3 (n-3) fatty acids.The 'paradox' makes much more sense to me now that I've seen this:
 It's from the same paper as the graphs in the last post. Note that it doesn't take much n-3 to get you to the asymptote. Here's another one that might interest you:
It's from the same paper as the graphs in the last post. Note that it doesn't take much n-3 to get you to the asymptote. Here's another one that might interest you: The finding in this graph is supported by the Lyon diet heart study, which I'll describe below. One more graph from a presentation by Dr. Lands, since I began by talking about the Inuit:
The finding in this graph is supported by the Lyon diet heart study, which I'll describe below. One more graph from a presentation by Dr. Lands, since I began by talking about the Inuit:
Cardiovascular disease mortality tracks well with the n-6 content of blood plasma, both across populations and within them. You can see modern Quebec Inuit have the same low rate of CVD mortality as the Japanese. The five red triangles are from MRFIT, a large American intervention trial. They represent the study participants divided into five groups based on their plasma n-6. Note that the average percentage of n-6 fatty acids is very high, even though the trial occurred in the 1970s! Since n-3 and n-6 fats compete for space in human tissue, it makes sense that the Inuit are protected from CVD by their high n-3 intake. [Update: I don't read too much into this graph because there are so may confounding variables. It's an interesting observation, but take it with a grain of salt.. SJG 2011].
Now for a little mechanism. Dr. Lands' hypothesis is that a high n-6 intake promotes a general state of inflammation in the body. The term 'inflammation' refers to the chronic activation of the innate immune system. The reason is that n-3 and n-6 fats are precursors to longer-chain signaling molecules called eicosanoids. In a nutshell, eicosanoids produced from n-6 fatty acids are more inflammatory and promote thrombosis (clotting) more than those produced from n-3 fatty acids. Dr. Lands is in a position to know this, since he was one of the main researchers involved in discovering these mechanisms. He points out that taking aspirin to 'thin' the blood and reduce inflammation (by inhibiting inflammatory eicosanoids) basically puts a band-aid over the problem caused by excess n-6 fats to begin with. [Update- this mechanism turns out not to be so straightforward. SJG 2011]
The Lyon Diet Heart Study assessed the effect of n-3 fat supplementation on CVD risk. The four-year intervention involved a number of diet changes designed to mimic the American Heart Association's concept of a "Mediterranean diet". The participants were counseled to eat a special margarine that was high in n-3 from alpha-linolenic acid. Overall PUFA intake decreased, mostly due to n-6 reduction, and n-3 intake increased relative to controls. The intervention caused a 70% reduction in cardiac mortality and a large reduction in all-cause mortality, a smashing success by any measure.
In a large five-year intervention trial in Japan, JELIS, patients who took EPA (a long-chain n-3 fatty acid) plus statins had 19% fewer cardiac events than patients taking statins alone. I don't know why you would give EPA by itself when it occurs with DHA and alpha-linolenic acid in nature, but it did nevertheless have a significant effect. Keep in mind that this trial was in Japan, where they already have a much better n-6/n-3 ratio than in Western nations.
In my opinion, what all the data (including a lot that I haven't included) point to is that a good n-6 to n-3 ratio may be important for vibrant health and proper development. In the next post, I'll talk about practical considerations for achieving a good ratio.
Thursday, September 4, 2008
Omega-3 Fats and Brain Development
Another interesting study that Dr. Hibbeln sent me is about the link between maternal seafood consumption and neurodevelopmental outcomes in children. The study is about as powerful as epidemiology gets, with an enrollment of 11,875 mothers.
The bottom line is short and sweet: compared to the children of mothers who ate 340 grams or more of fish per week, children whose mothers ate very little fish had an increased risk of low verbal intelligence, poor social behavior, poor motor skills, poor communication skills, and poor social development. These associations remained after adjusting for 28 potential confounders, including social status, level of education, stressful life events, smoking, alcohol, and several others.
In support of this association, in another study the four-year-old children of mothers who were given DHA and arachidonic acid supplements had higher IQs than those given "placebo" (corn oil). There have been a number of trials of varying quality that have shown varying results with n-3 supplementation, so I'll leave you to decide what you think of this. A 2007 review I found on n-3 supplementation and brain development states that "the evidence for potential benefits of LCPUFA [long-chain polyunsaturated fatty acid] supplementation is promising but yet inconclusive".
I do think it's interesting to note that the brain has the highest concentration of long-chain n-3 fats of any organ, and eating n-3 fats in the form of fish, fish oil or cod liver oil increases the amount in tissues. Eating too much n-6 depletes the brain of DHA and adversely affects neuron development in piglets. n-3 deficiency affects the release of serotonin (a neurotransmitter) in rat brains.
Put it all together, including the data from the last two posts, and I think there's some evidence that a good balance of n-3 to n-6 fatty acids is important for optimal brain function and perhaps development.
The bottom line is short and sweet: compared to the children of mothers who ate 340 grams or more of fish per week, children whose mothers ate very little fish had an increased risk of low verbal intelligence, poor social behavior, poor motor skills, poor communication skills, and poor social development. These associations remained after adjusting for 28 potential confounders, including social status, level of education, stressful life events, smoking, alcohol, and several others.
In support of this association, in another study the four-year-old children of mothers who were given DHA and arachidonic acid supplements had higher IQs than those given "placebo" (corn oil). There have been a number of trials of varying quality that have shown varying results with n-3 supplementation, so I'll leave you to decide what you think of this. A 2007 review I found on n-3 supplementation and brain development states that "the evidence for potential benefits of LCPUFA [long-chain polyunsaturated fatty acid] supplementation is promising but yet inconclusive".
I do think it's interesting to note that the brain has the highest concentration of long-chain n-3 fats of any organ, and eating n-3 fats in the form of fish, fish oil or cod liver oil increases the amount in tissues. Eating too much n-6 depletes the brain of DHA and adversely affects neuron development in piglets. n-3 deficiency affects the release of serotonin (a neurotransmitter) in rat brains.
Put it all together, including the data from the last two posts, and I think there's some evidence that a good balance of n-3 to n-6 fatty acids is important for optimal brain function and perhaps development.
Tuesday, September 2, 2008
The Omega Ratio
The theory advanced by Dr. Lands and Hibbeln is that the ratio of omega-6 to omega-3 fatty acids in the diet is the crucial factor for mental and physical health, rather than the absolute amount of each. Omega-6 and -3 fats are essential long-chain polyunsaturated fatty acids. The number refers to the position of the double bond near the methyl end of the carbon chain.
The ratio of omega-6 to omega-3 (hereafter, n-6 and n-3) in the diet determines the ratio in tissues. Since these molecules have many cellular roles, it doesn't stretch the imagination that they could have an effect on health. Hunter-gatherer and healthy non-industrial cultures typically have a favorable ratio of n-6 to n-3, 2:1 or less. In the US, the ratio is currently about 17:1 due to modern vegetable oils.
DHA, a long-chain n-3 fatty acid, is concentrated in neuronal synapses (the connections between neurons) and is required for the normal functioning of neurons. n-6 fats compete with n-3 fats for space in cellular membranes (which have a fixed amount of total polyunsaturated fat), so a high intake of n-6 fats, particularly linoleic acid, displaces n-3 fatty acids. Lower tissue levels of DHA and total n-3 correlate with measures of hostility in cocaine addicts. Feeding mice a diet high in linoleic acid increases aggressive behavior, and increses the likelihood of rats to kill mice.
If the ratio of n-6 to n-3 in the diet predicts psychiatric problems, we'd expect to see an association with n-3 intake as well. Let's take a look:
 This is homicide mortality vs. n-3 intake for 24 countries, published here. The association is significant (p> 0.001) even without correcting for n-6 intake. Of course, one could see this as a cloud of points with a few well-placed outliers. Here are some closer associations from the same paper:
This is homicide mortality vs. n-3 intake for 24 countries, published here. The association is significant (p> 0.001) even without correcting for n-6 intake. Of course, one could see this as a cloud of points with a few well-placed outliers. Here are some closer associations from the same paper:
 It's clear that both a high n-6 intake and a low n-3 intake correlate with negative psychiatric outcomes. Together, the data are consistent with the hypothesis that the ratio of n-6 to n-3 impacts brain function. Dr. Hibbeln and Dr. Lands do not claim that this ratio is the sole determinant of psychiatric problems, only that it is a factor.
It's clear that both a high n-6 intake and a low n-3 intake correlate with negative psychiatric outcomes. Together, the data are consistent with the hypothesis that the ratio of n-6 to n-3 impacts brain function. Dr. Hibbeln and Dr. Lands do not claim that this ratio is the sole determinant of psychiatric problems, only that it is a factor.
Now to address the big criticism that was brought up by very astute readers of the last post, namely, that the data were purely correlative. Believe me, I wouldn't even have posted on this topic if I didn't have intervention data to back it up. In addition to the animal data I mentioned above, here are more studies that support a causal role of fatty acid balance in psychiatric problems:
The ratio of omega-6 to omega-3 (hereafter, n-6 and n-3) in the diet determines the ratio in tissues. Since these molecules have many cellular roles, it doesn't stretch the imagination that they could have an effect on health. Hunter-gatherer and healthy non-industrial cultures typically have a favorable ratio of n-6 to n-3, 2:1 or less. In the US, the ratio is currently about 17:1 due to modern vegetable oils.
DHA, a long-chain n-3 fatty acid, is concentrated in neuronal synapses (the connections between neurons) and is required for the normal functioning of neurons. n-6 fats compete with n-3 fats for space in cellular membranes (which have a fixed amount of total polyunsaturated fat), so a high intake of n-6 fats, particularly linoleic acid, displaces n-3 fatty acids. Lower tissue levels of DHA and total n-3 correlate with measures of hostility in cocaine addicts. Feeding mice a diet high in linoleic acid increases aggressive behavior, and increses the likelihood of rats to kill mice.
If the ratio of n-6 to n-3 in the diet predicts psychiatric problems, we'd expect to see an association with n-3 intake as well. Let's take a look:
 This is homicide mortality vs. n-3 intake for 24 countries, published here. The association is significant (p> 0.001) even without correcting for n-6 intake. Of course, one could see this as a cloud of points with a few well-placed outliers. Here are some closer associations from the same paper:
This is homicide mortality vs. n-3 intake for 24 countries, published here. The association is significant (p> 0.001) even without correcting for n-6 intake. Of course, one could see this as a cloud of points with a few well-placed outliers. Here are some closer associations from the same paper: It's clear that both a high n-6 intake and a low n-3 intake correlate with negative psychiatric outcomes. Together, the data are consistent with the hypothesis that the ratio of n-6 to n-3 impacts brain function. Dr. Hibbeln and Dr. Lands do not claim that this ratio is the sole determinant of psychiatric problems, only that it is a factor.
It's clear that both a high n-6 intake and a low n-3 intake correlate with negative psychiatric outcomes. Together, the data are consistent with the hypothesis that the ratio of n-6 to n-3 impacts brain function. Dr. Hibbeln and Dr. Lands do not claim that this ratio is the sole determinant of psychiatric problems, only that it is a factor. Now to address the big criticism that was brought up by very astute readers of the last post, namely, that the data were purely correlative. Believe me, I wouldn't even have posted on this topic if I didn't have intervention data to back it up. In addition to the animal data I mentioned above, here are more studies that support a causal role of fatty acid balance in psychiatric problems:
- EPA supplementation (a long-chain n-3 fatty acid) reduced aggression and depression in a group of women with borderline personality disorder.
- DHA supplementation improved aggression in young Thai students.
- n-3 supplementation improved symptoms of bipolar disorder.
- EPA supplementation improved symptoms of unipolar depression.
- n-3 supplementation improved perinatal depression.
- n-3 supplementation improved symptoms of major depression.
- DHA and EPA supplementation reduced suicidal behaviors and improved markers of well-being in patients with recurrent self-harm.
- n-3 supplementation decreased anger and anxiety in substance abusers.
Monday, September 1, 2008
Vegetable Oil and Homicide
One of the major dietary changes that has accompanied the downward slide of American health is the replacement of animal fats with industrially processed vegetable oils. Soybean oil, corn oil, cottonseed oil and other industrial creations have replaced milk and meat fat in our diet, while total fat consumption has remained relatively constant. The result is that we're eating a lot more polyunsaturated fat than we were just 30 years ago, most of it linoleic acid (omega-6). Corn oil may taste so bad it inspires you to violence, but its insidiousness goes beyond the flavor. Take a look:

 This figure is from a paper that Dr. Joe Hibbeln sent me recently, of which he is the first author. This followed an interesting e-mail conversation with Robert Brown, author of Omega Six: the Devil's Fat. He put me in touch with Dr. Hibbeln and Dr. William Lands (NIH, NIAAA), both of whom warn of the dangers of excessive linoleic acid consumption from modern vegetable oils. Dr. Lands has been researching the relationship between dietary fat and inflammation since the 1970s, and has been a critic of modern vegetable oils for just as long. Both Dr. Hibbeln and Dr. Lands were very generous in sending me a number of their papers. The figure above shows the homicide rate vs. linoleic acid consumption of five countries over the course of 40 years. Each point represents one year in one country. The U.S. has the distinction of being in the upper right.
This figure is from a paper that Dr. Joe Hibbeln sent me recently, of which he is the first author. This followed an interesting e-mail conversation with Robert Brown, author of Omega Six: the Devil's Fat. He put me in touch with Dr. Hibbeln and Dr. William Lands (NIH, NIAAA), both of whom warn of the dangers of excessive linoleic acid consumption from modern vegetable oils. Dr. Lands has been researching the relationship between dietary fat and inflammation since the 1970s, and has been a critic of modern vegetable oils for just as long. Both Dr. Hibbeln and Dr. Lands were very generous in sending me a number of their papers. The figure above shows the homicide rate vs. linoleic acid consumption of five countries over the course of 40 years. Each point represents one year in one country. The U.S. has the distinction of being in the upper right.
I asked Dr. Hibbeln how he selected the five countries, and he told me the selection criteria were 1) available homicide and linoleic acid consumption statistics, 2) "first world" countries, and 3) countries representing a diversity of linoleic acid intakes. I'm satisfied that there was probably not a significant selection bias.
What's interesting about the graph is that not only does the homicide rate track with linoleic acid consumption across countries, but it also tracks within countries over time. For example, here is the same graph of the US alone:

And here is the UK, which doesn't suffer as much from the confounding factor of firearm availability:

I don't think we can draw any solid conclusions from this, but it is worth noting that epidemiological associations don't get much better. In the next few posts, I'll explore the data from intervention trials that support the hypothesis that excessive omega-6 consumption, and insufficient omega-3 consumption, cause serious problems for psychiatric and physical health.
 This figure is from a paper that Dr. Joe Hibbeln sent me recently, of which he is the first author. This followed an interesting e-mail conversation with Robert Brown, author of Omega Six: the Devil's Fat. He put me in touch with Dr. Hibbeln and Dr. William Lands (NIH, NIAAA), both of whom warn of the dangers of excessive linoleic acid consumption from modern vegetable oils. Dr. Lands has been researching the relationship between dietary fat and inflammation since the 1970s, and has been a critic of modern vegetable oils for just as long. Both Dr. Hibbeln and Dr. Lands were very generous in sending me a number of their papers. The figure above shows the homicide rate vs. linoleic acid consumption of five countries over the course of 40 years. Each point represents one year in one country. The U.S. has the distinction of being in the upper right.
This figure is from a paper that Dr. Joe Hibbeln sent me recently, of which he is the first author. This followed an interesting e-mail conversation with Robert Brown, author of Omega Six: the Devil's Fat. He put me in touch with Dr. Hibbeln and Dr. William Lands (NIH, NIAAA), both of whom warn of the dangers of excessive linoleic acid consumption from modern vegetable oils. Dr. Lands has been researching the relationship between dietary fat and inflammation since the 1970s, and has been a critic of modern vegetable oils for just as long. Both Dr. Hibbeln and Dr. Lands were very generous in sending me a number of their papers. The figure above shows the homicide rate vs. linoleic acid consumption of five countries over the course of 40 years. Each point represents one year in one country. The U.S. has the distinction of being in the upper right.I asked Dr. Hibbeln how he selected the five countries, and he told me the selection criteria were 1) available homicide and linoleic acid consumption statistics, 2) "first world" countries, and 3) countries representing a diversity of linoleic acid intakes. I'm satisfied that there was probably not a significant selection bias.
What's interesting about the graph is that not only does the homicide rate track with linoleic acid consumption across countries, but it also tracks within countries over time. For example, here is the same graph of the US alone:

And here is the UK, which doesn't suffer as much from the confounding factor of firearm availability:

I don't think we can draw any solid conclusions from this, but it is worth noting that epidemiological associations don't get much better. In the next few posts, I'll explore the data from intervention trials that support the hypothesis that excessive omega-6 consumption, and insufficient omega-3 consumption, cause serious problems for psychiatric and physical health.
Subscribe to:
Posts (Atom)